Clinical fetaures
•4% of melanoma cases in the USA
•Predominantly affects sun damaged skin of the elderly
•Malar region, nose, temple, forehead
•Less of back of hand
•Variably pigmented slowly growing macule with irregular borders & variable pigmentation
•Papule or nodule formation indicates invasive tumor
•Hypopigmentation is strongly suggestive of regression


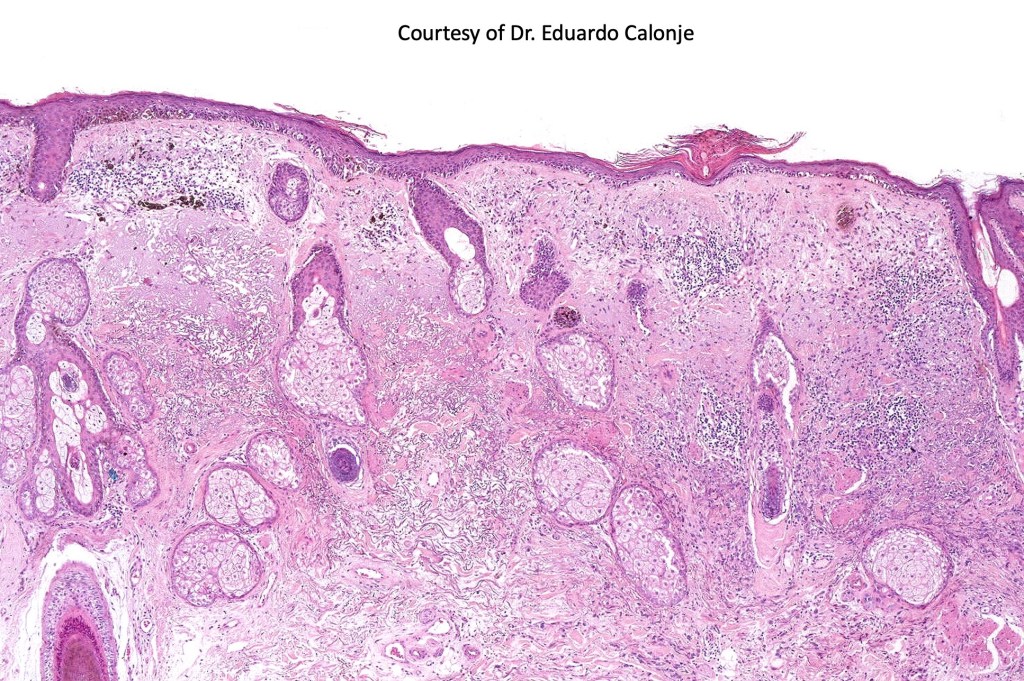
Histological features & immunohistochemstry
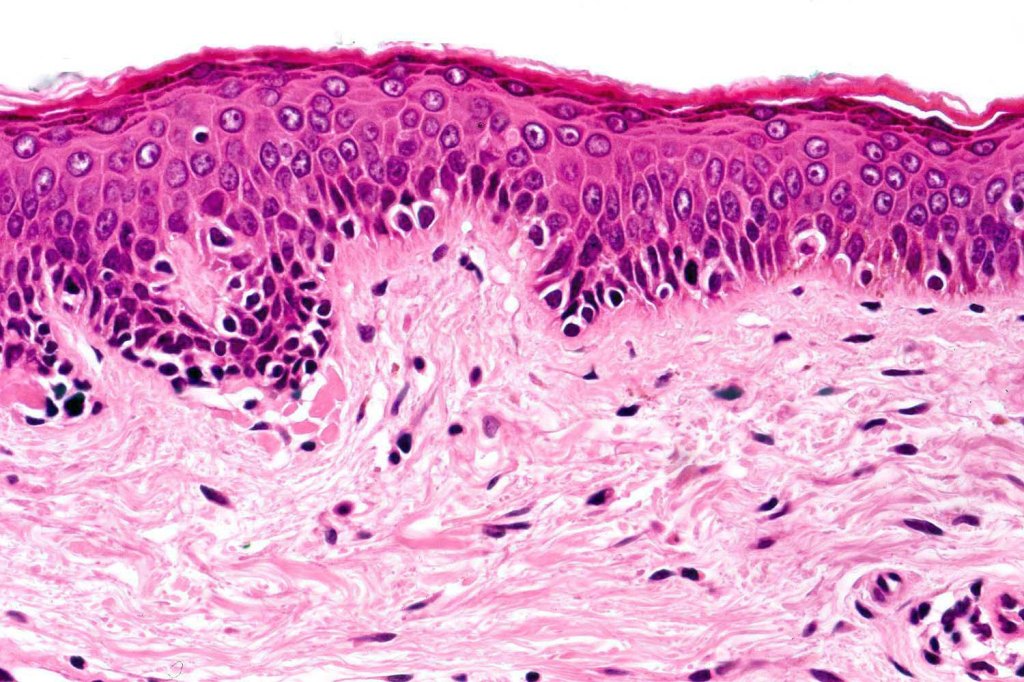
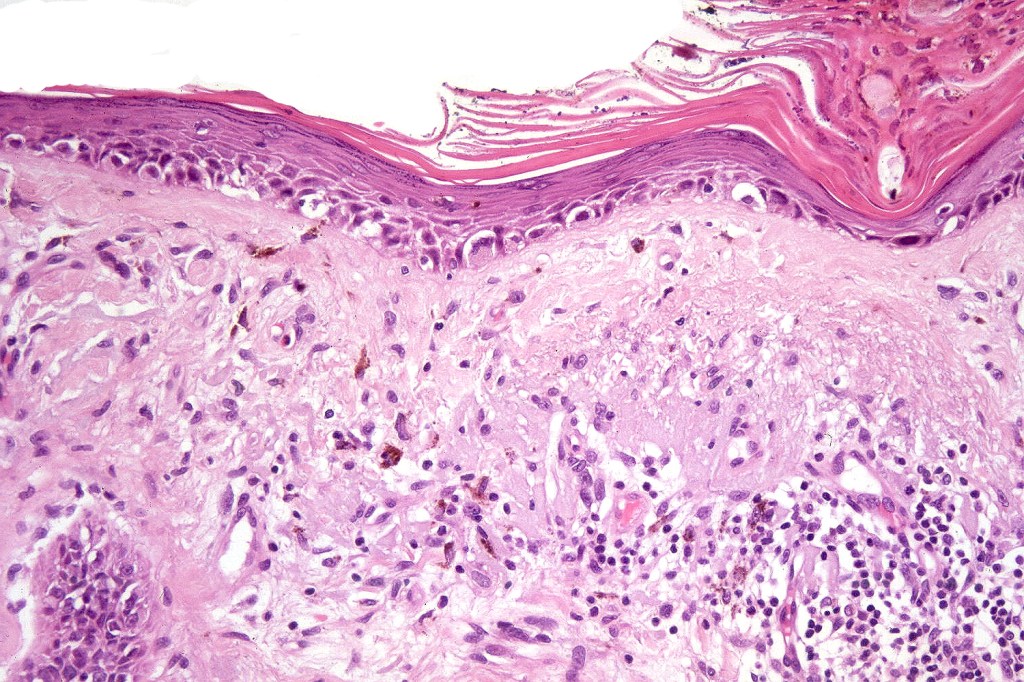
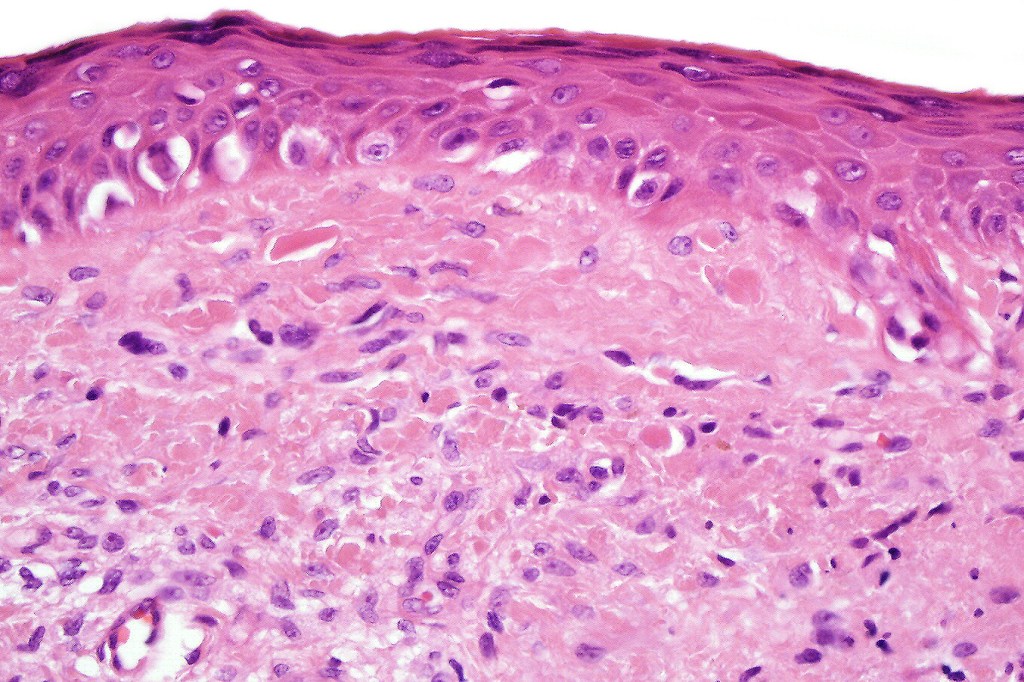
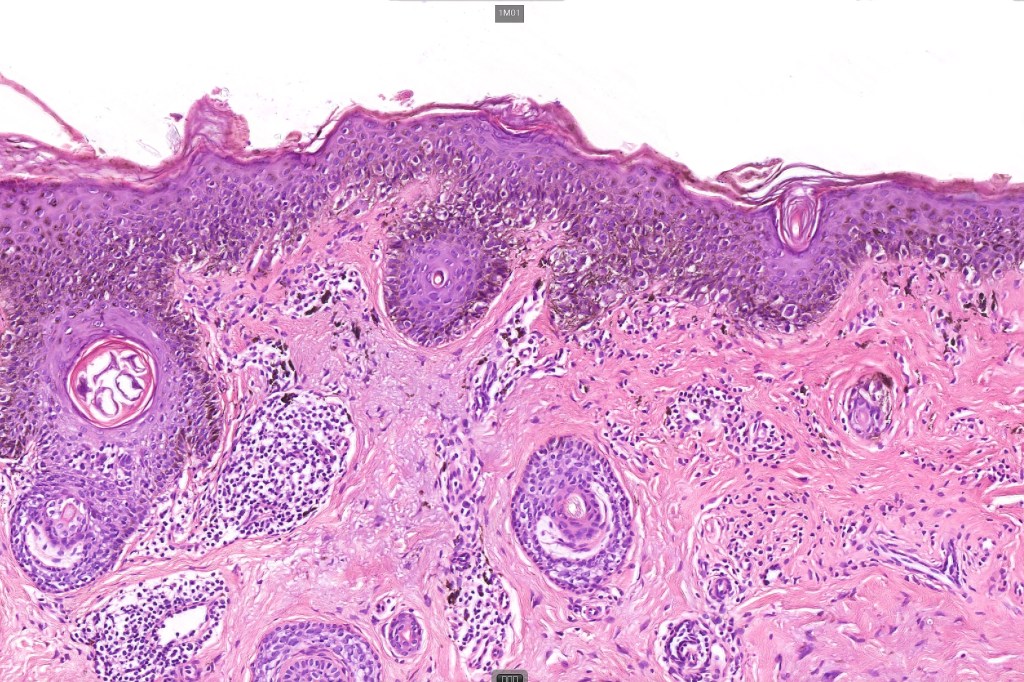
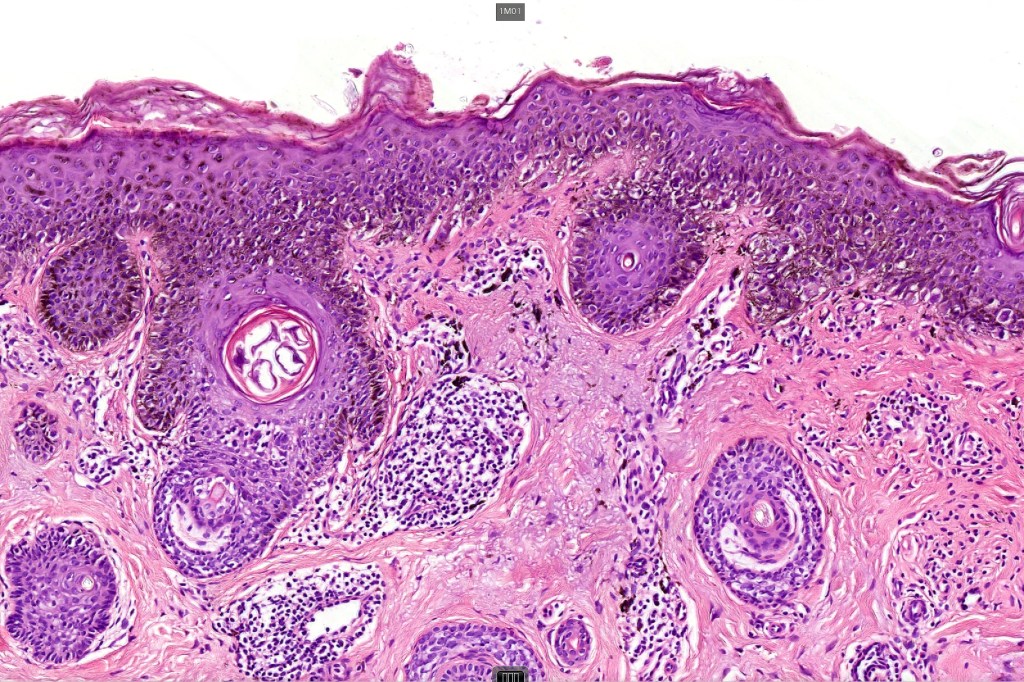
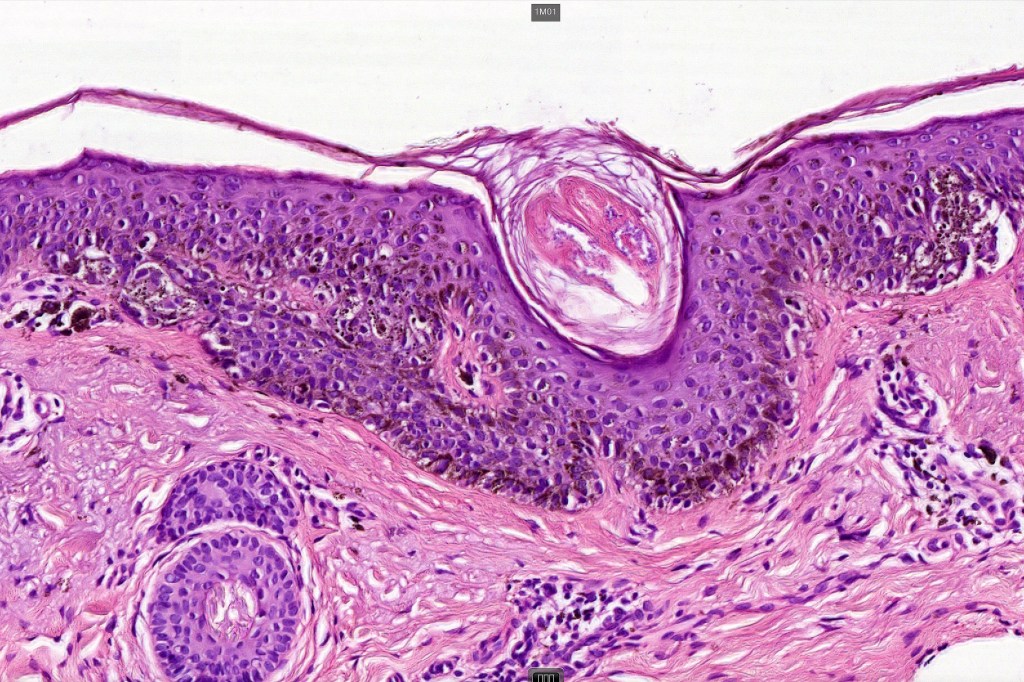
•Epidermal atrophy & solar elastosis
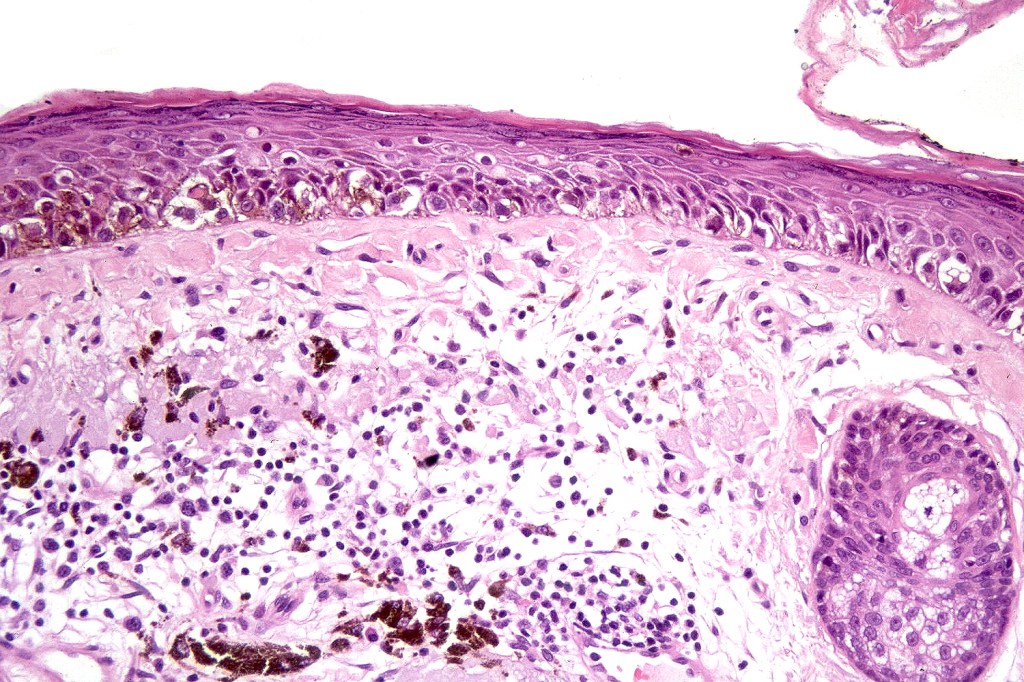
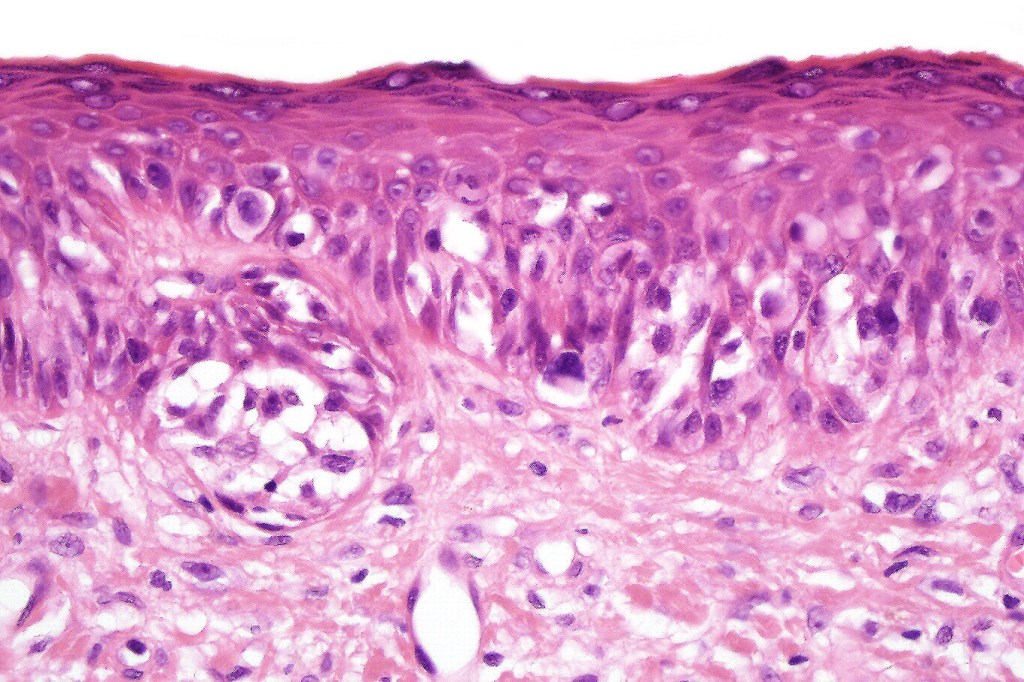
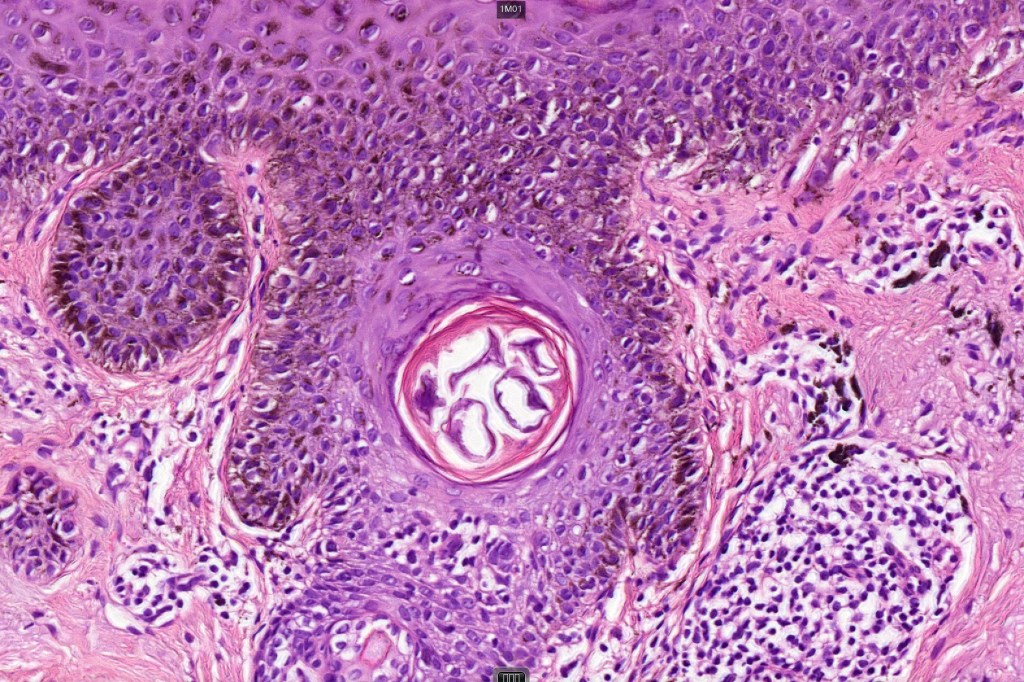
•Atypical melanocytes located predominantly along the basal layer of the epidermis, singly, in short arrays or extensively involving the whole epidermis
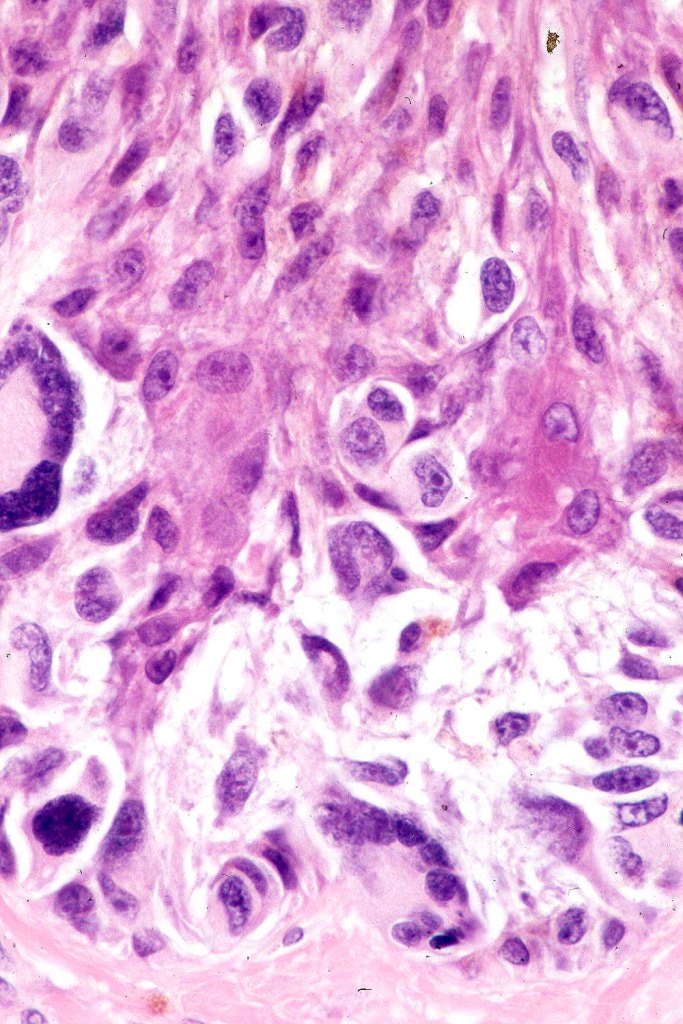
•Cytoplasmic retraction artifact, nuclear hyperchromatism with irregular borders
•Multinucleate giant cells
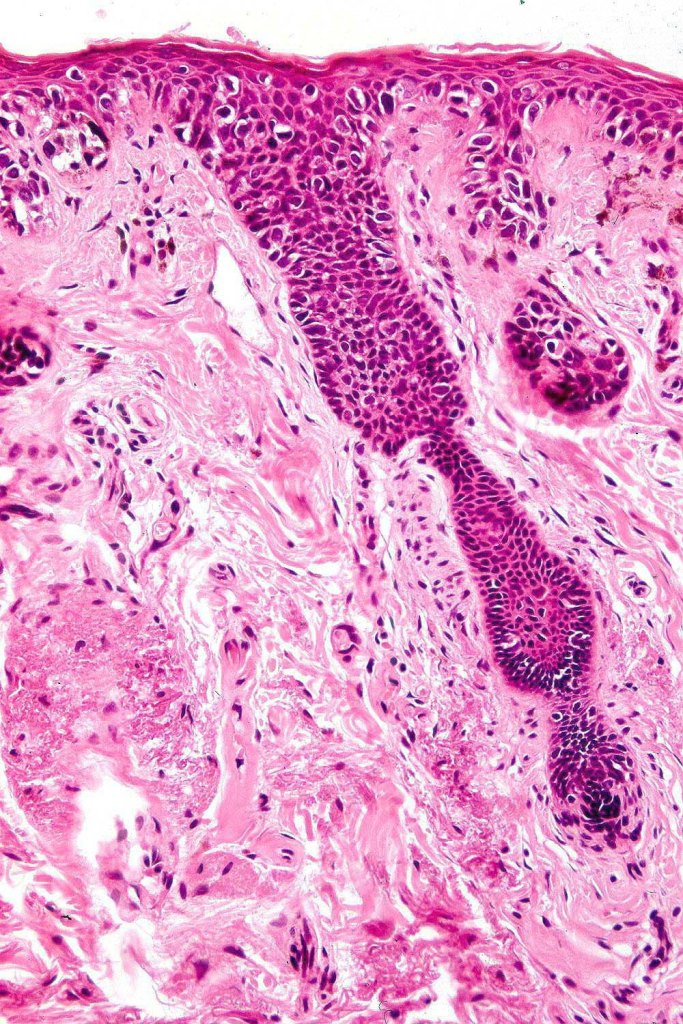
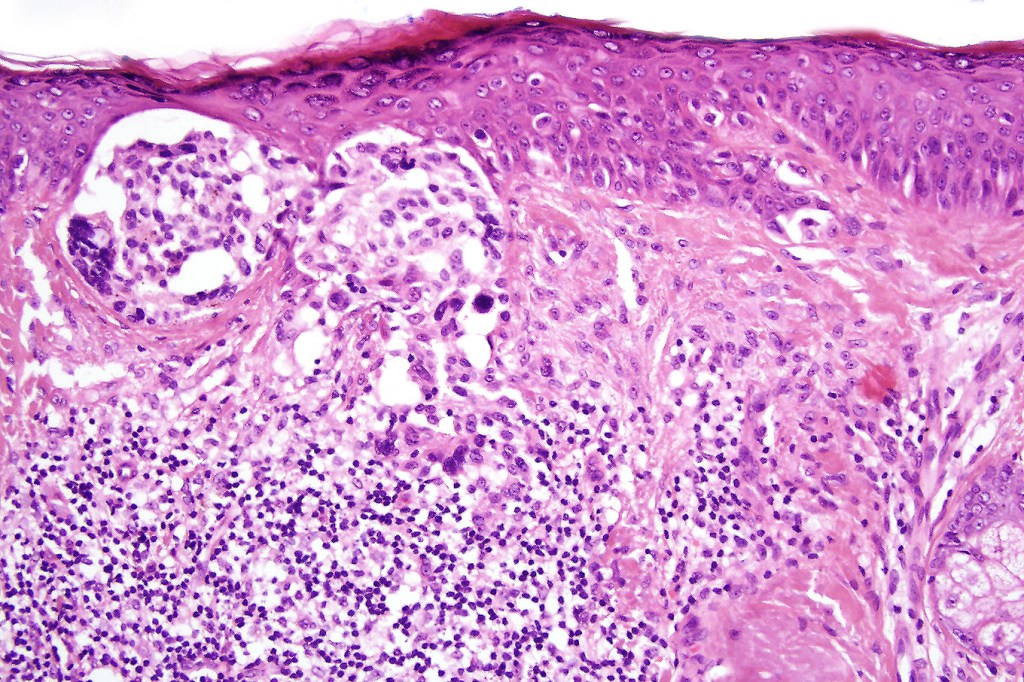
•Nest formation present in more advanced cases
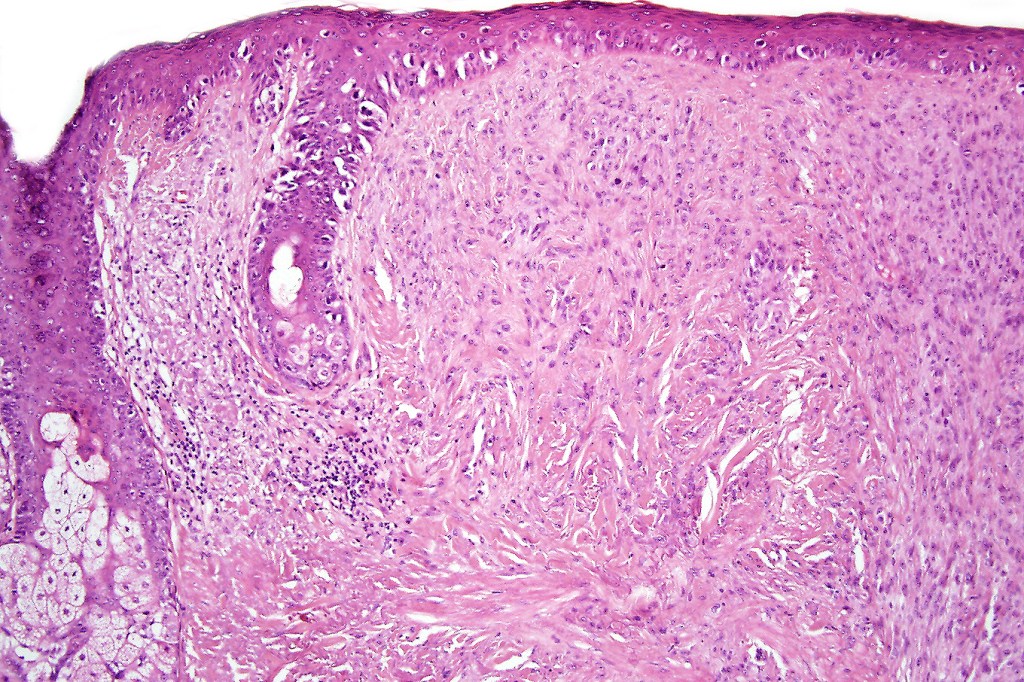
•Adnexal involvement
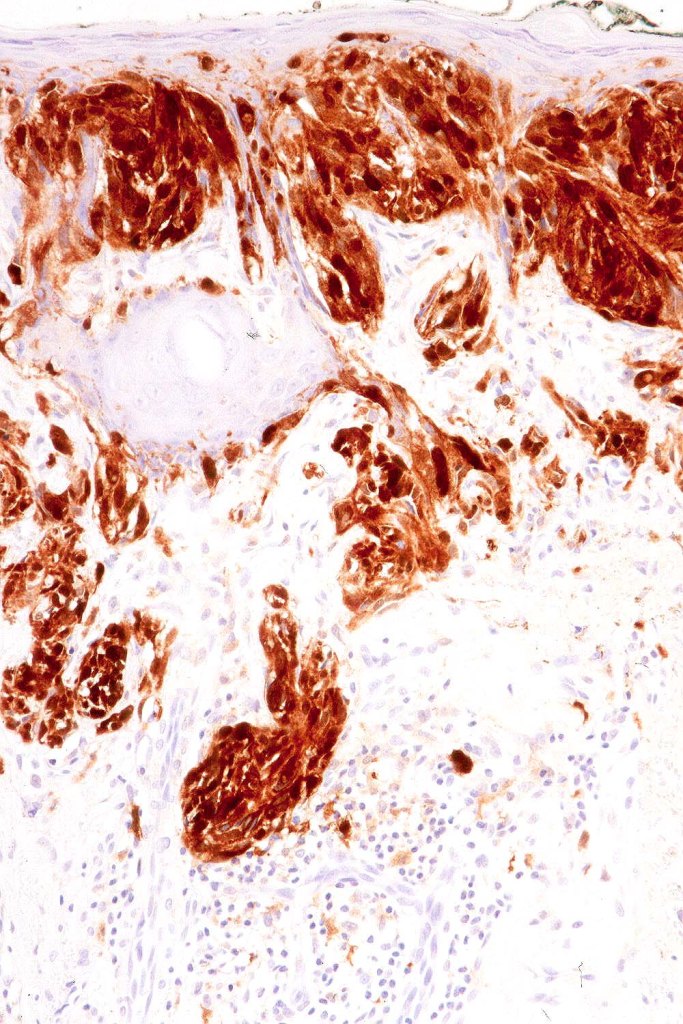
•Dense melanin pigmentation may affect the whole epidermis making it difficult to determine which cells are melanocytes & which are keratinocytes! DAB-lablled antibodies should be avoided as they can be impossible to interpret
•Mitoses can be conspicuous
•Pagetoid spread
•Dermal melanophages & lymphocytic infiltration
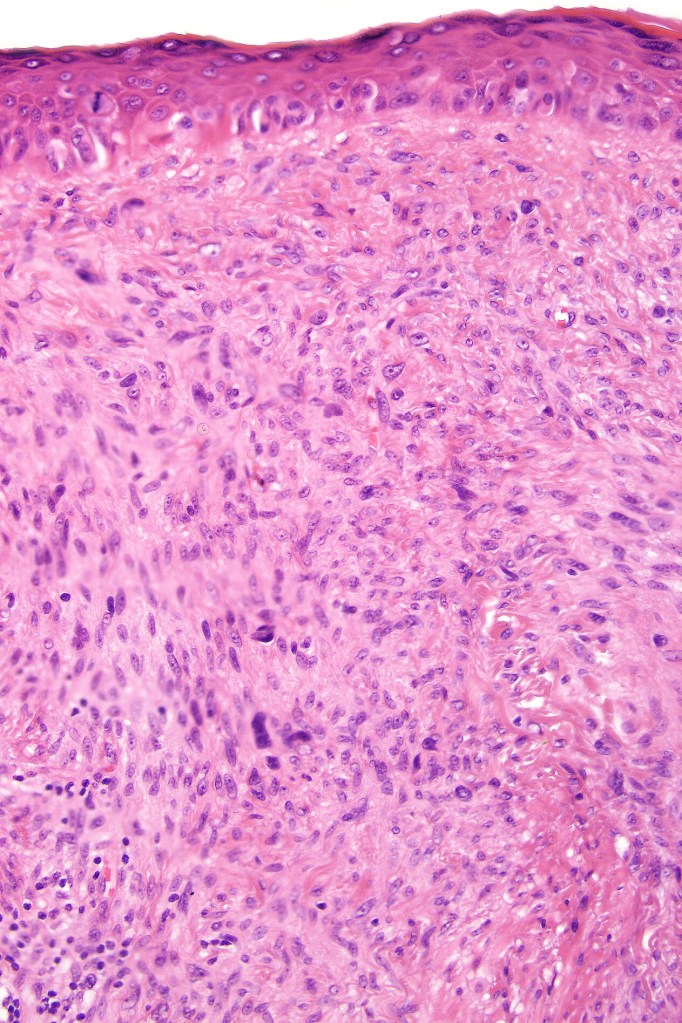
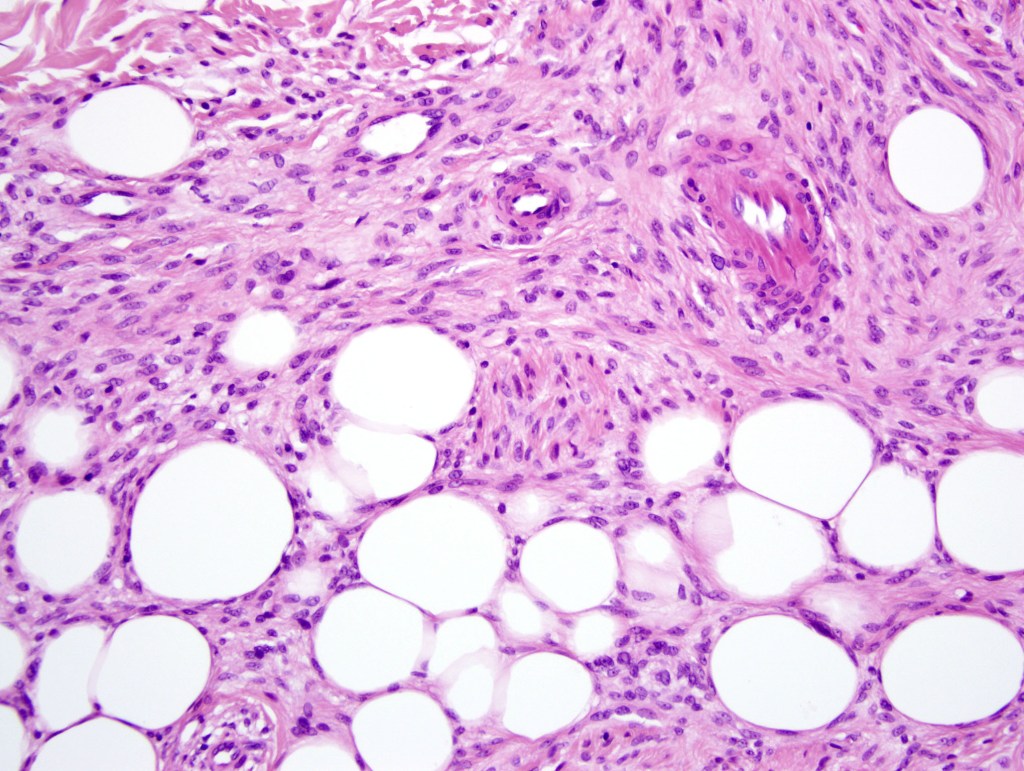
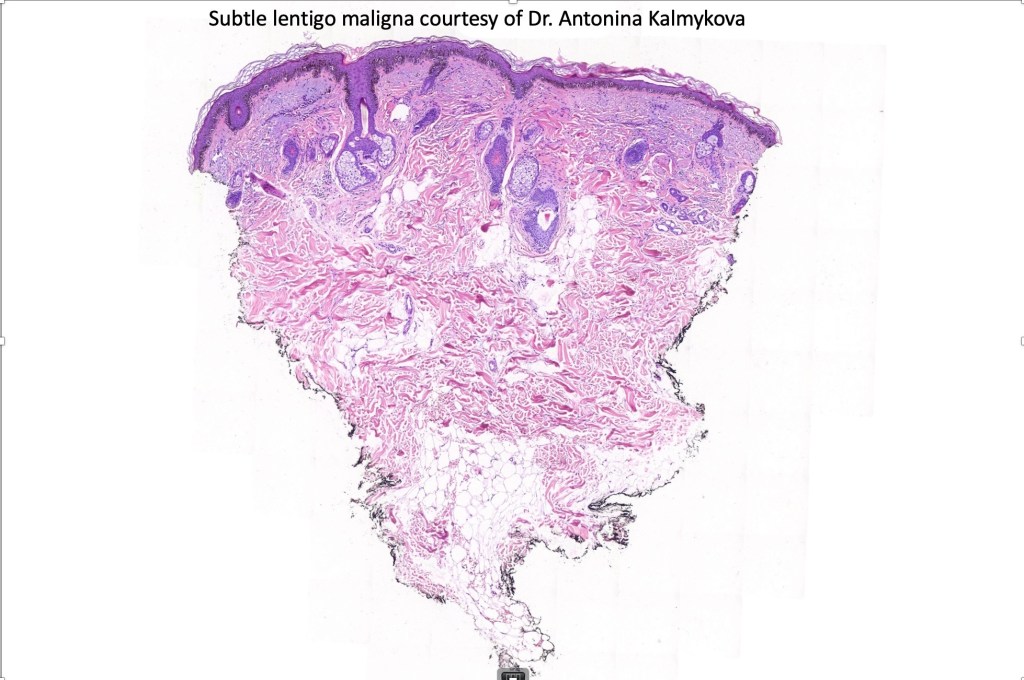
•Invasive tumor (lentigo maligna melanoma) typically characterized by a spindle cell population
•Invasion can be subtle and may require immunohistochemistry
•Desmoplastic and neurotropic melanoma in a significant number of cases
. SOX10, Melan A, MITF, PRAME, p53+ve

























Differential diagnosis
Melanocytic (atypical) hyperplasia of sun damaged skin is the most important differential diagnosis. This can be extremely challenging, particularly when examining the margins for completeness of excision. The problem is even worse with MOH’s surgery specimens. Points of distinction include predominace of single cells, abscence of linear arrays of atypical melanocytes, absence of mitoses, nests and Pagetoid spread.


Leave a comment