Dystrophic epidermolysis bullosa (DEB) develops as a consequence of mutations in COL7A1. This results in defective or absent anchoring fibrils. As a consequence the skin is susceptible to shearing blisters with even minor trauma. Repeated blistering and ulceration complicated by severe scarring results. Squamous cell carcinoma (SCC) is most often encountered on the extremities. Current information on the pathogenesis of this tumor in the setting of DEB can be found in the review article below. Although SCC is of major importance in patients with recessive disease (RDEB), patients with generalized dominant disease (DDEB) are also at high risk.


Clinical features
•A very common complication and cause of severe morbidity and high mortality; squamous carcinoma is the most common cause of death in severely affected patients
•Up to 90% of patients with severe recessive dystrophic disease will eventually develop tumors
•Mean age of onset 29.5 years
•The extremities & bony prominences are most often affected
•Oral & esophageal tumors
•Generally, arise in long standing ulcers associated with marked scarring
•Metastases develop in around 40% of patients





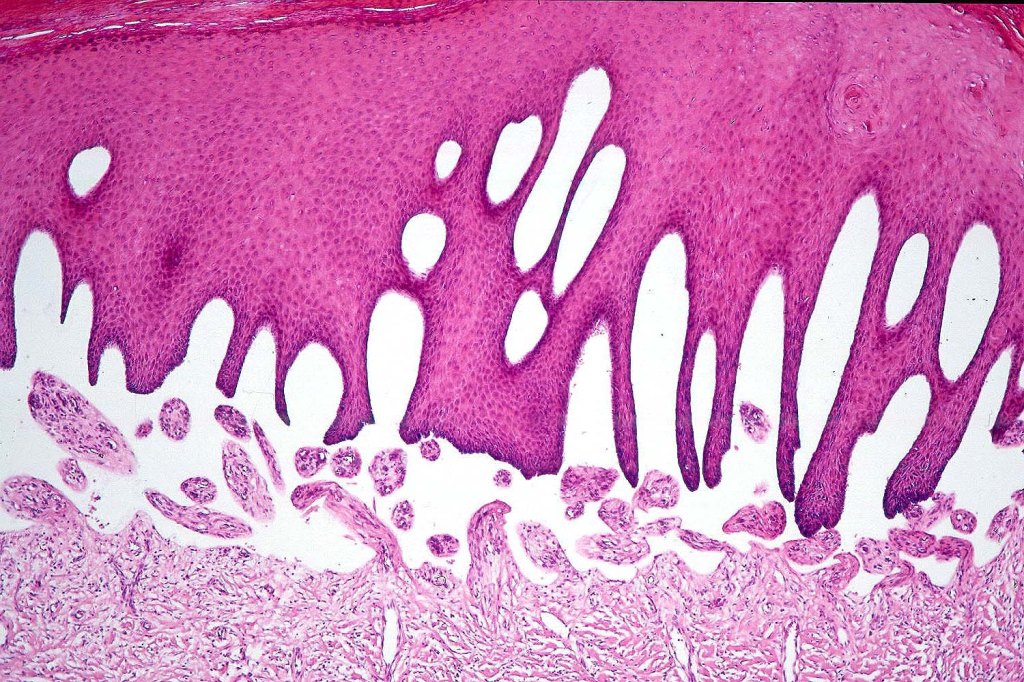
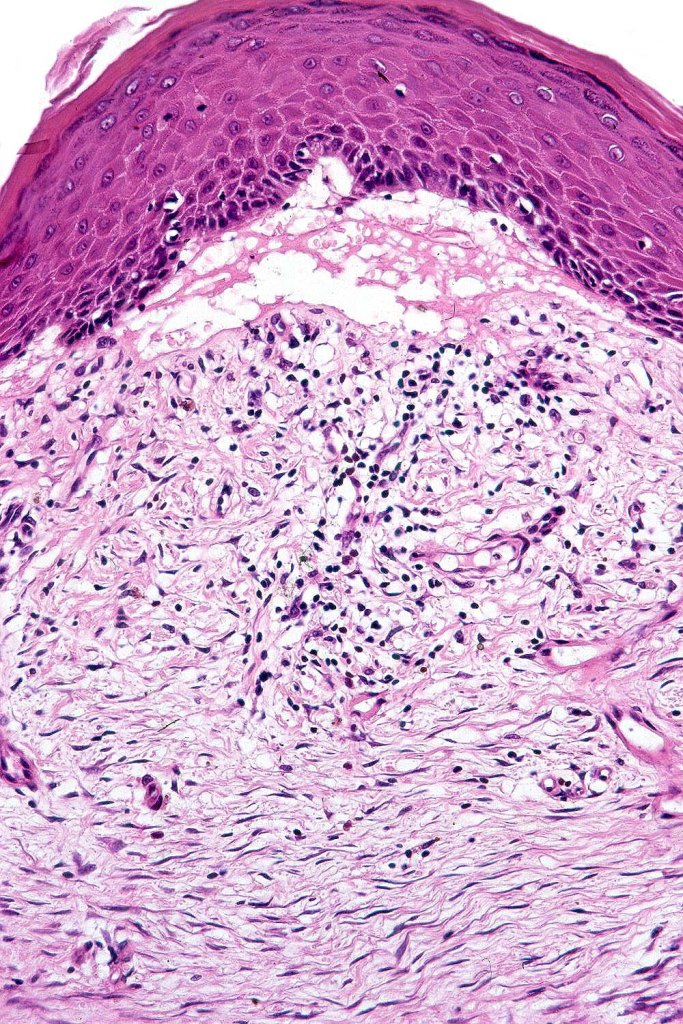
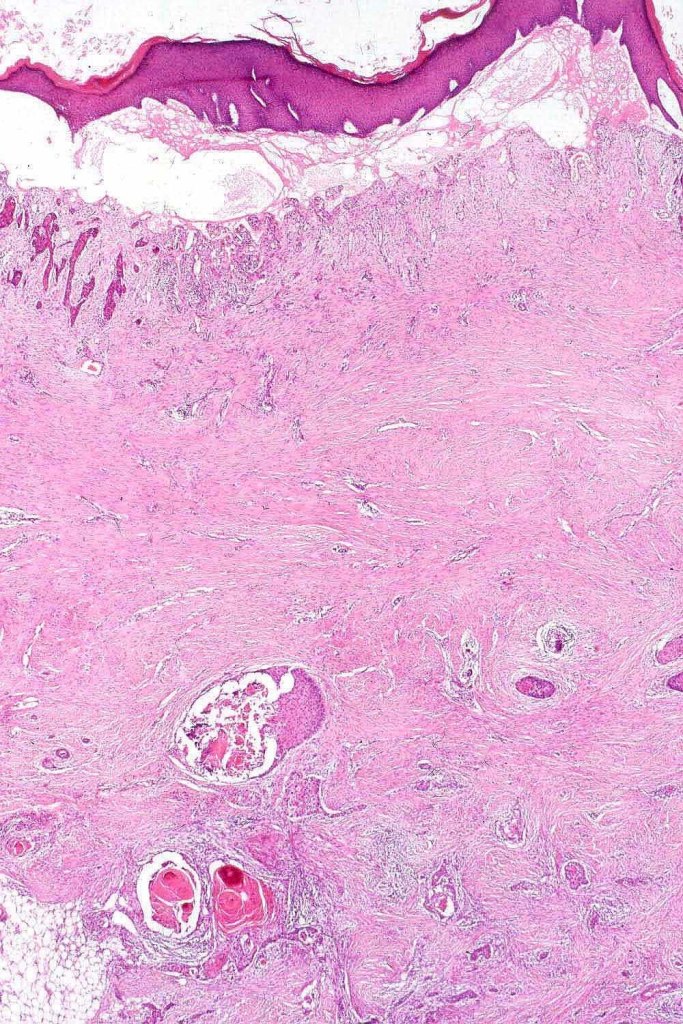
Histological features
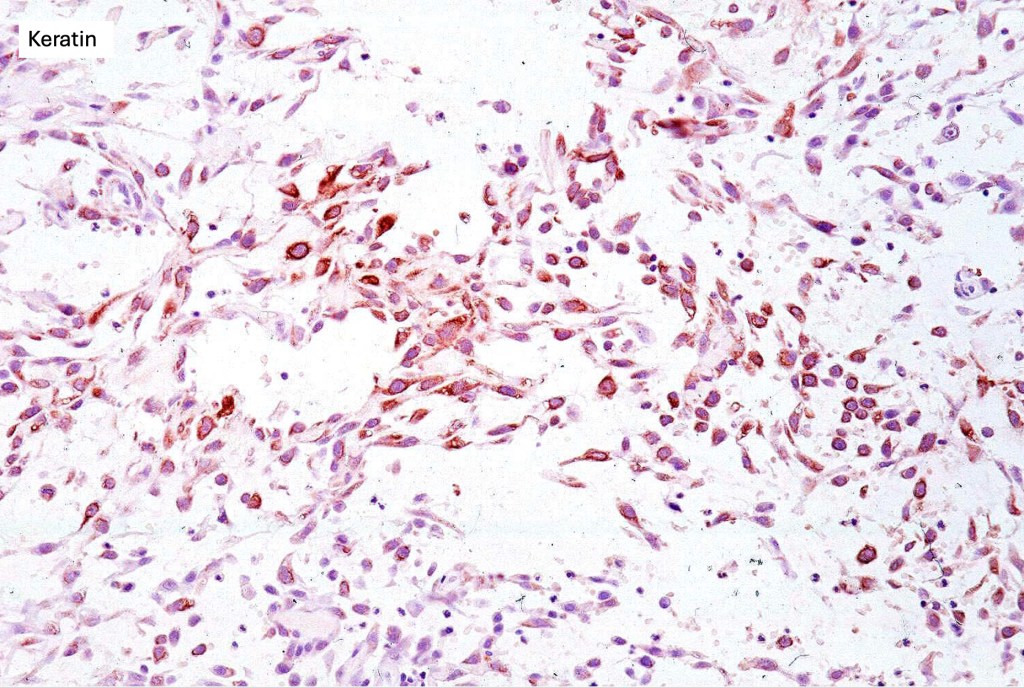
•Generally, tumors are well differentiated although they can later develop a more poorly differentiated morphology
•Keratoses may represent a precursor & sometimes histological distinction between very marked epidermal hyperplasia (pseudoepitheliomatous) and early SCC can be problematical (personal observation)






Leave a comment