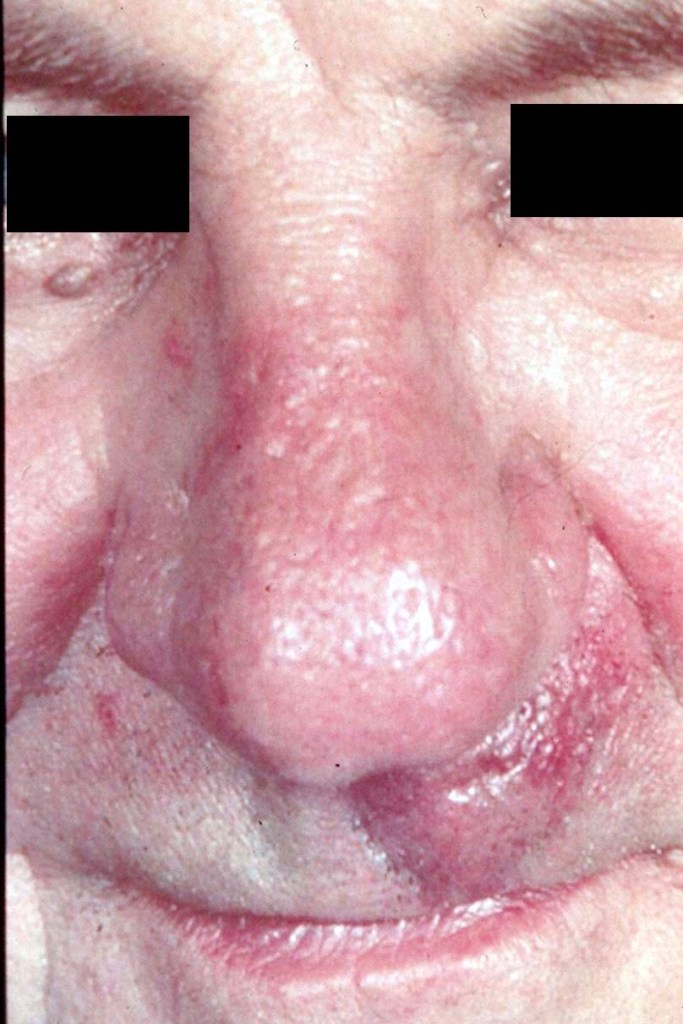
Clinical features
- 6-90 years (4th-7th decade), M=F
- Caucasians ++
- Nasolabial & periorbital regions
- Slowly growing firm 0.5-2.0 cm plaque or nodule with deceptive borders
- Central dell often present
- Pain, burning or paresthesia
- The clinical “edge” of the lesion is very deceptive. At surgery the tumor invariably is much larger
- Mohs surgery is an excellent treatment option
- The image below shows a recurrent tumor



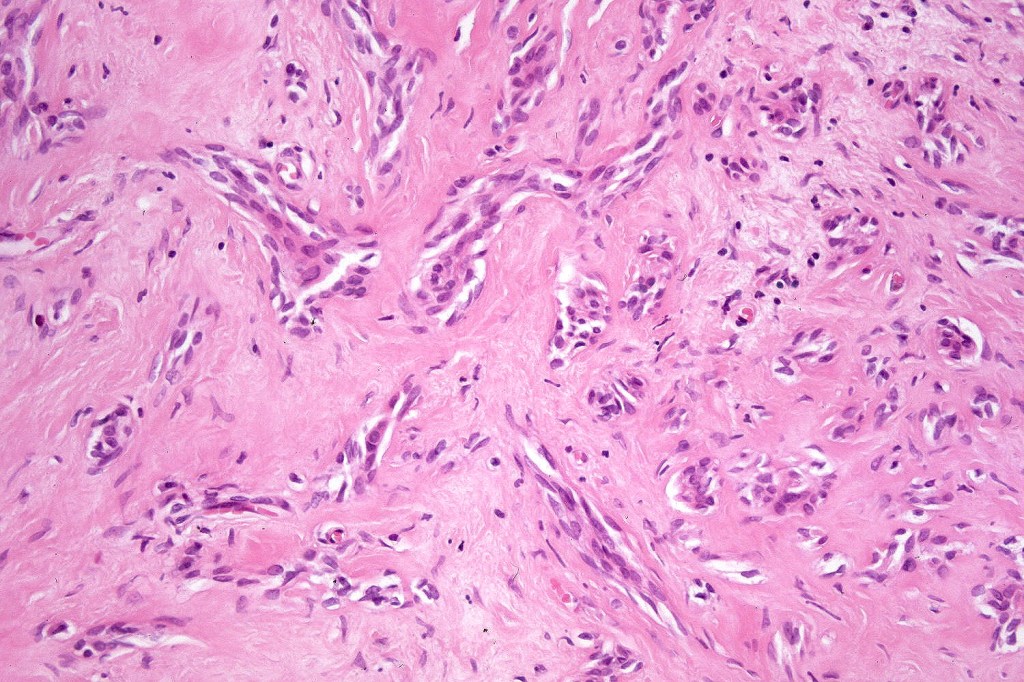
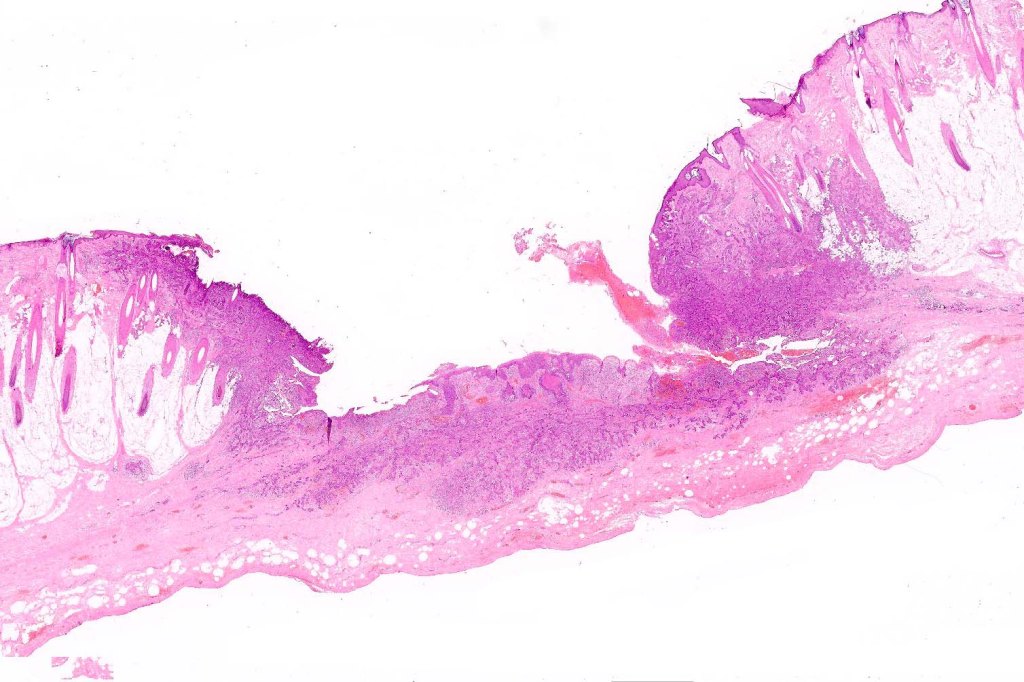
Histology


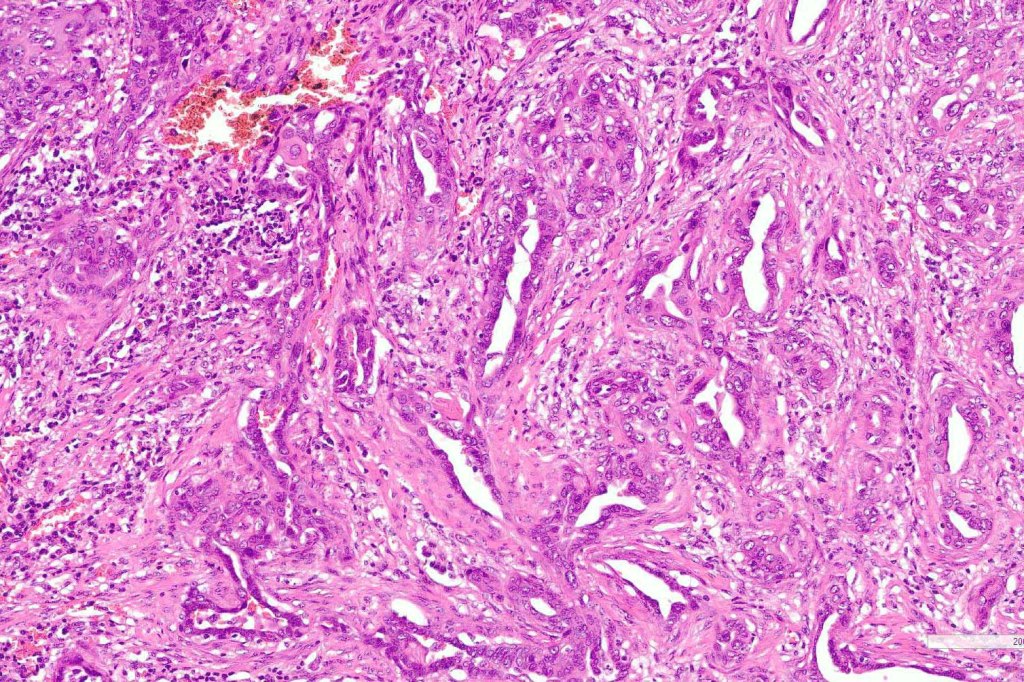
Histological features
- Poorly circumscribed
- ? sweat gland or sweat gland & follicular differentiation
- Rarely sebaceous differentiation (6 cases)
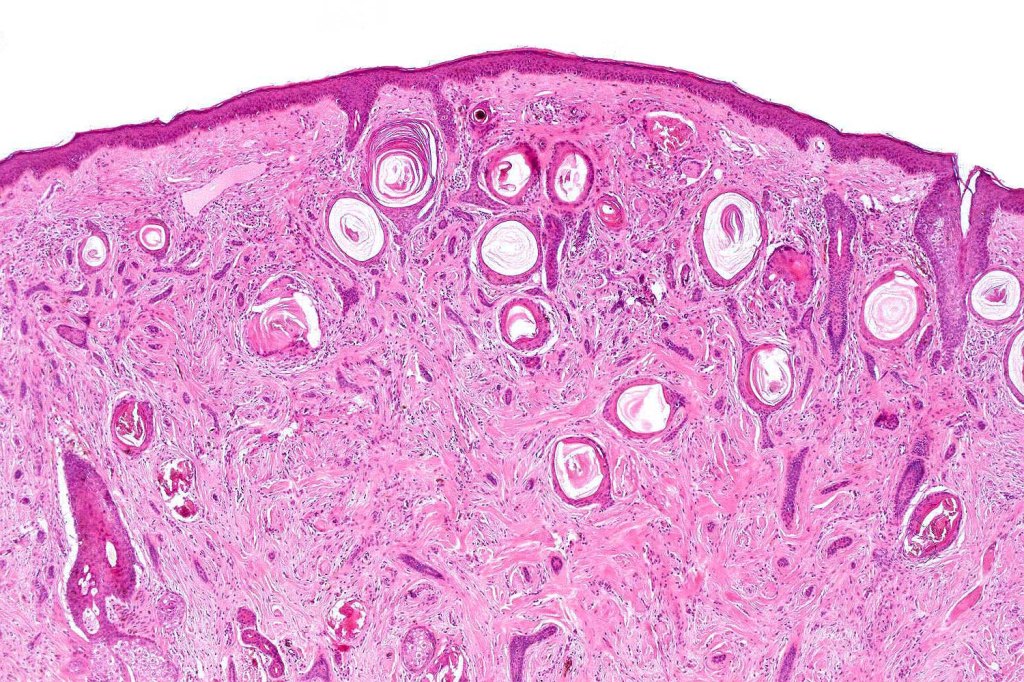
- Keratocysts with epidermoid keratinization
- Pilar keratinization is also sometimes present in the deeper reaches
- Clear cell change (if very marked, clear cell variant)
- Solid narrow epithelial strands (sometimes predominates and keratocysts absent (eccrine epithelioma, syringoid eccrine carcinoma)
- Minimal pleomorphism
- Mitoses very sparse or absent
- Ductal differentiation
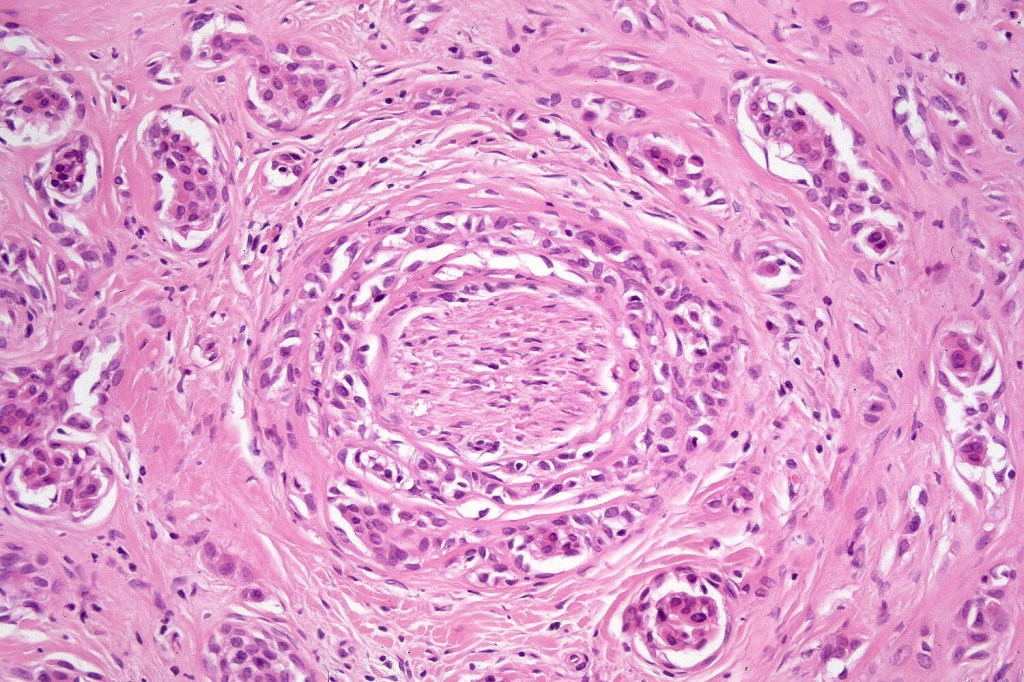
- Invariable perineural infiltration*
- Dense fibrous stroma
- Solid variant
- High grade variant








Immunohistochemistry
- AE1/AE3 +ve
- CK15 -ve
- EMA & CEA show ductal differentiation
- BerEP4 –ve
- Low Ki67 expression
- Mutation in TP53 & loss of CDK2NA & CDKN2B (one case with metastases)

Prognosis
- Recurrences: 15-60%
- Recurrences may be greatly reduced with Mohs surgery
- MAC rarely involves nodes, exceptionally systemic spread (3)
- Radiotherapy is contra-indicated (if the tumor recurs, the dense fibrous stroma is worsened making surgery virtually impossible)
- Chemotherapy in systemic disease (carboplatin & paclitaxel)- one case
Differential diagnosis
- Desmoplastic trichoepithelioma*
- Trichoadenoma
- Squamoid eccrine ductal carcinoma
- Desmoplastic/sclerosing squamous cell carcinoma
- Morpheaform BCC
- Syringoma
- SCC with MAC-like differentiation
Desmoplastic trichoepithelioma
- Slowly growing white or yellow indurated plaque 3-8 mm in diameter
- Usually asymptomatic
- Face & neck ++, young adults
- 4F:1M
- May have a central dell
- High recurrence rate
- Confined to dermis*
- Comprises keratocysts and narrow epithelial strands typically showing a follicular connection
- Calcification often present
- No pleomorphism & mitoses generally absent
- No ductal differentiation (role of EMA and CEA)
- Perineural infiltration has recently been described (may account for the high recurrence rate*

Trichoadenoma
- Rare solitary 3-50 mm nodule on face and buttocks in adults
- Linear & verrucous variants
- Differentiated towards infundibulum (Images courtesy of Professor Jonhan Ho, KiKo)
- Cysts showing infundibular keratinization
- Calcification & foreign body giant cell reaction
- CK20 +ve Merkel cells


Squamoid eccrine ductal carcinoma
- Sun-damaged skin
- Elderly
- Face and neck++
- Males>Females
- Ulcerated
- nodule/plaque
- Often arises in an AK (Images courtey of Dr. Bipim Thingujam)
- Superficially shows features of squamous carcinoma with an epidermal origin
- Deep aspect- adenocarcinoma
- Pleomorphism often marked & mitoses generally numerous
- Recurrences-25% (series of 20 cases)
- Metastases 13% (1 with distant spread)


Leave a comment