Clinical features
•Very rare
•M=F
•Age range 18-91
•Axilla>>scalp, eyelid, ear, anogenital region, chest, lip & wrist
•Slowly growing sometimes ulcerated nodule or plaque
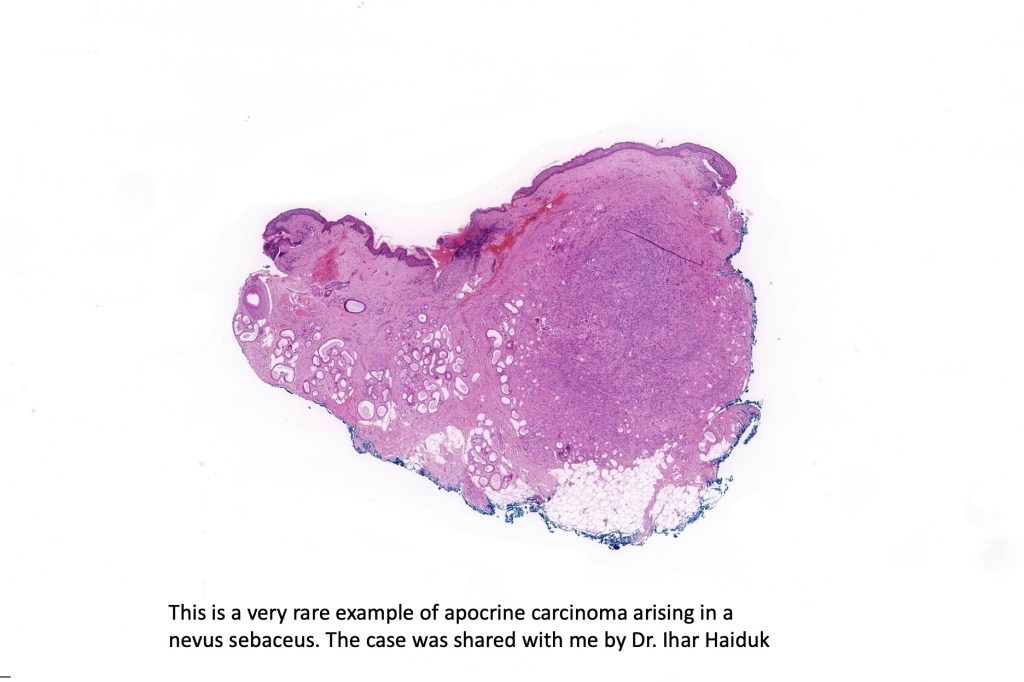
•Rarely develops in a nevus sebaceus or complicates a benign precursor apocrine tumor
•Often slowly growing and fairly indolent although high grade variants are not uncommon
•Metastases to lymph nodes (50%), lung and bone
•Recurrence rate 28%
•Median survival: 51.5 months
•Nodal and distant metastasis are poor prognosis indicators
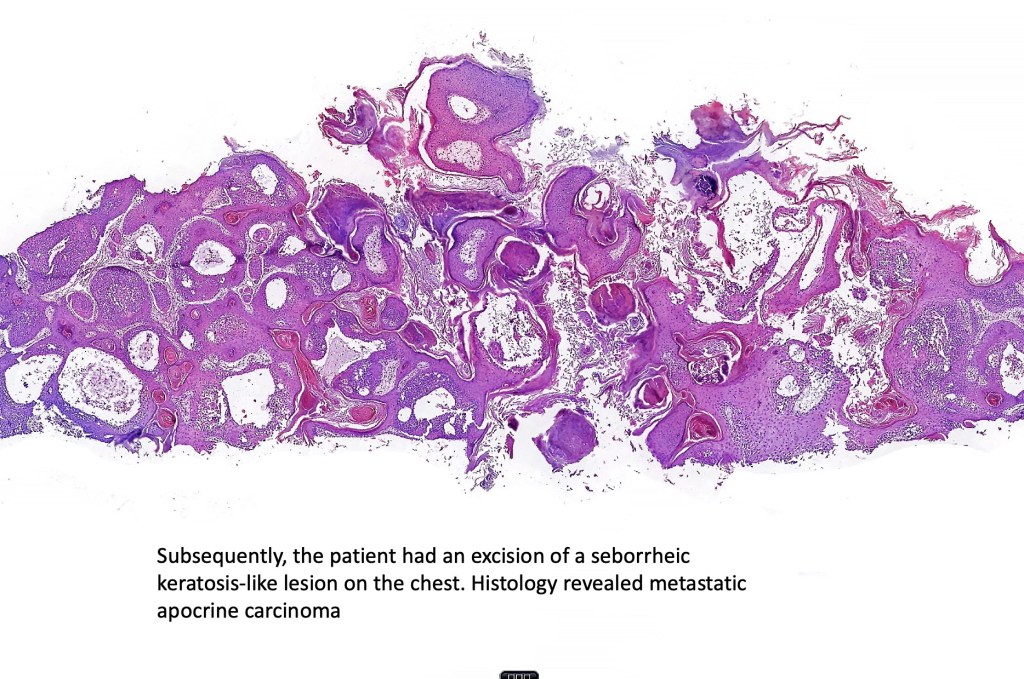
•Before accepting a tumor as being a cutaneous primary, the presence of an apocrine carcinoma elsewhere (particularly the breast) must always be excluded
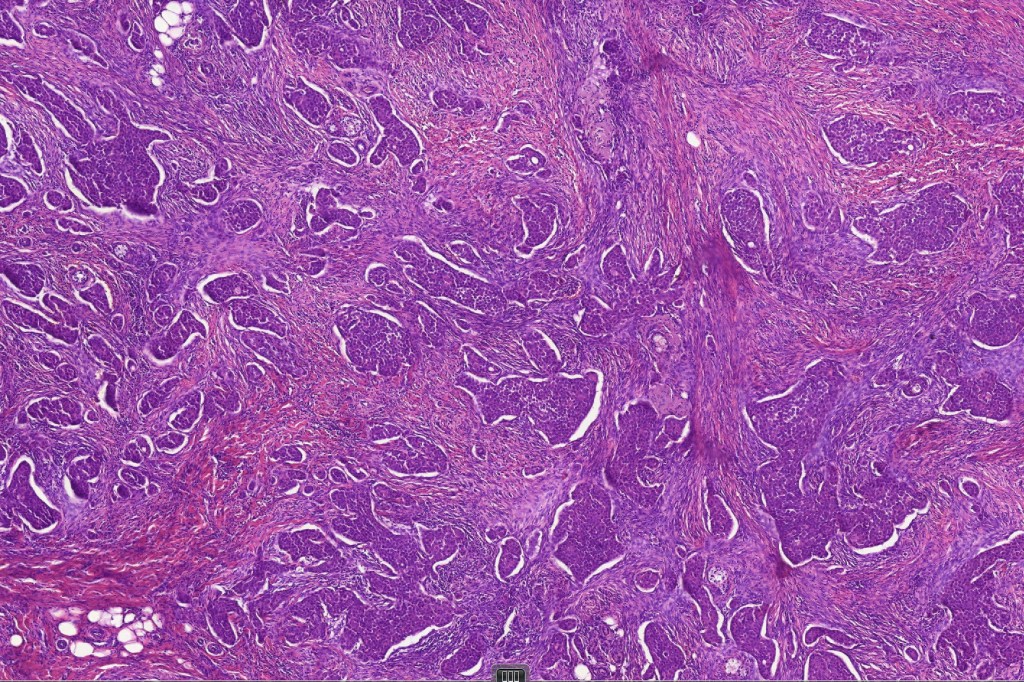
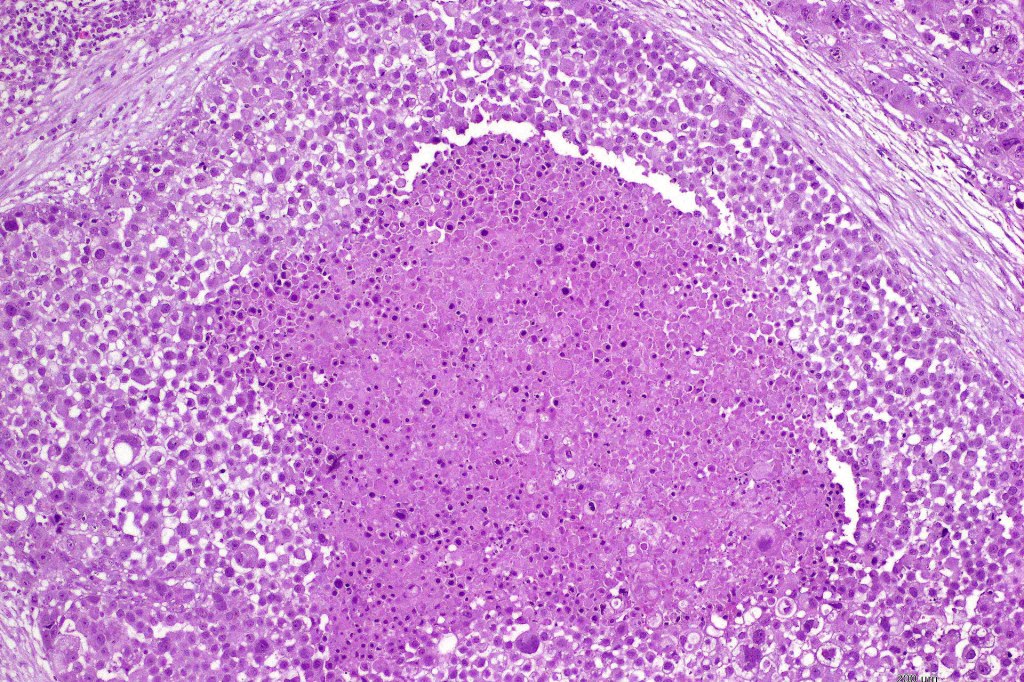
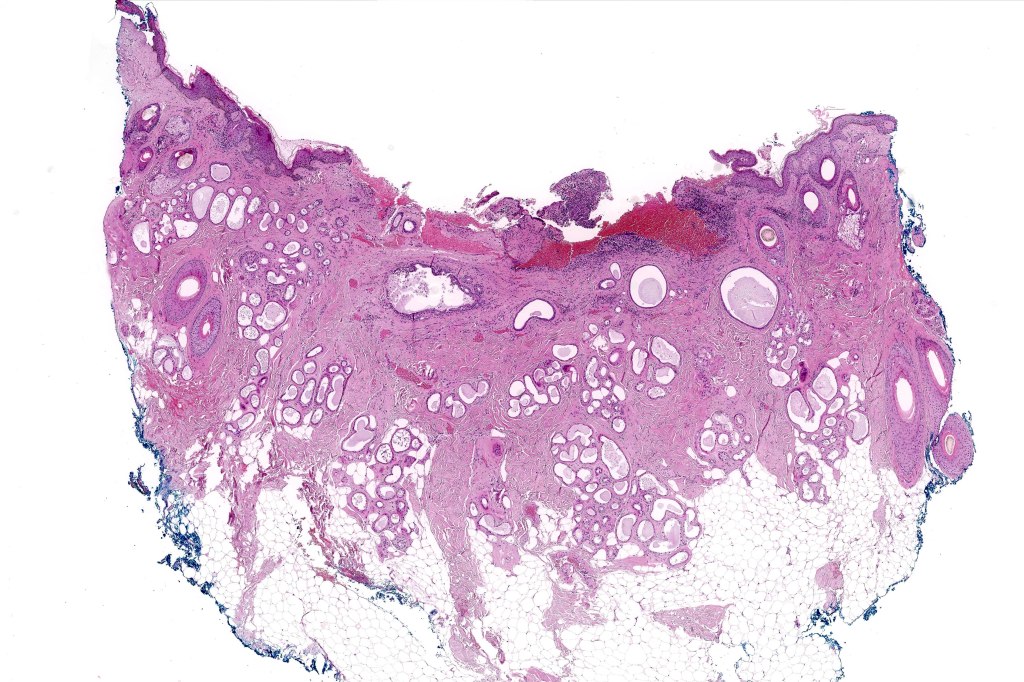
Histological features
•May develop in a background of a benign precursor tumor or exceptionally nevus sebaceus
•Poorly circumscribed tumor nodule with invasive border
•Rarely cystic
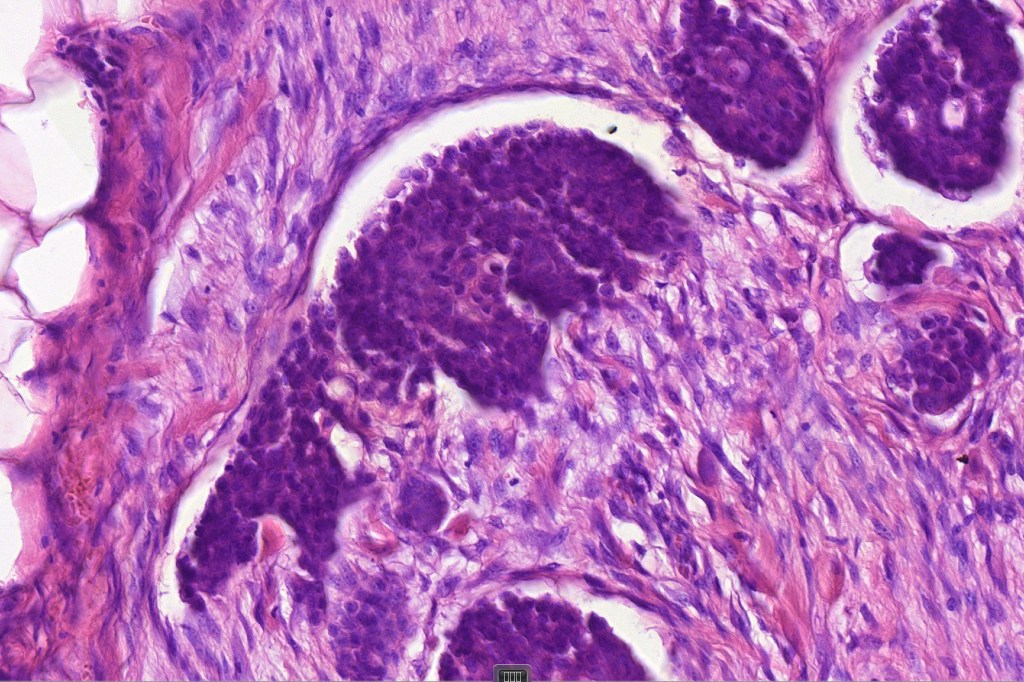
•Variable glandular, tubular, papillary, tubulo-papillary, diffuse and solid growth patterns
•Can be associated with overlying Paget’s disease
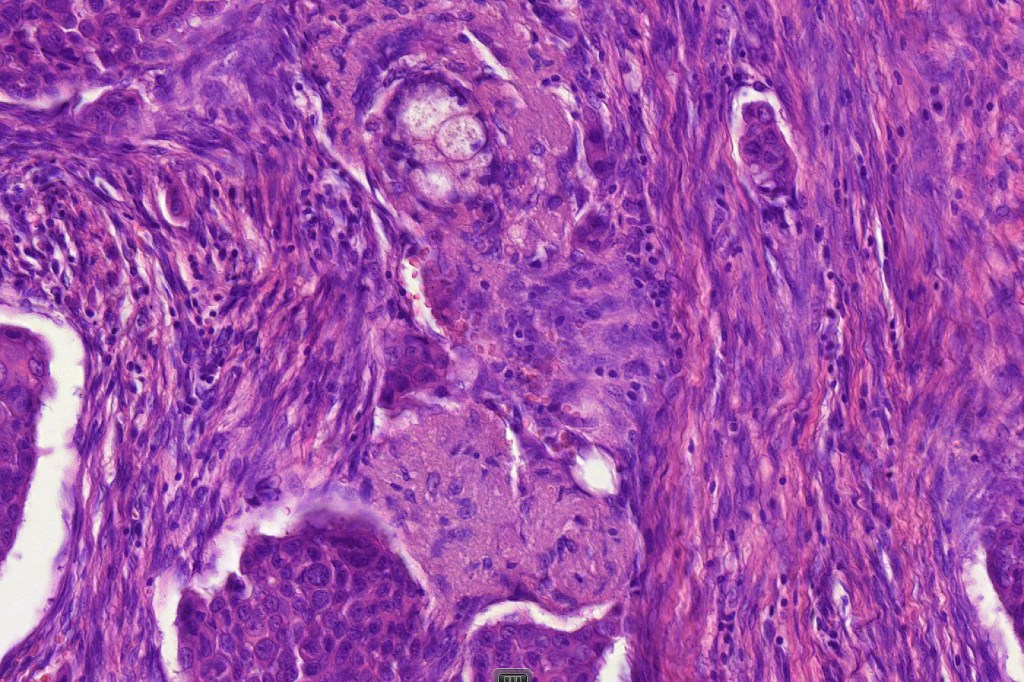
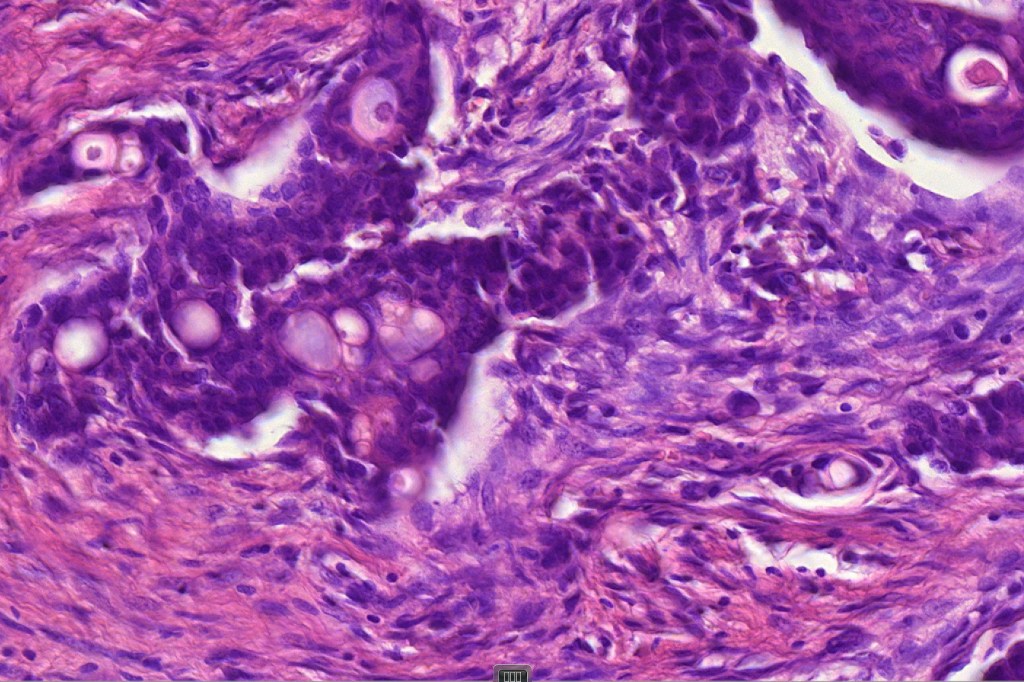
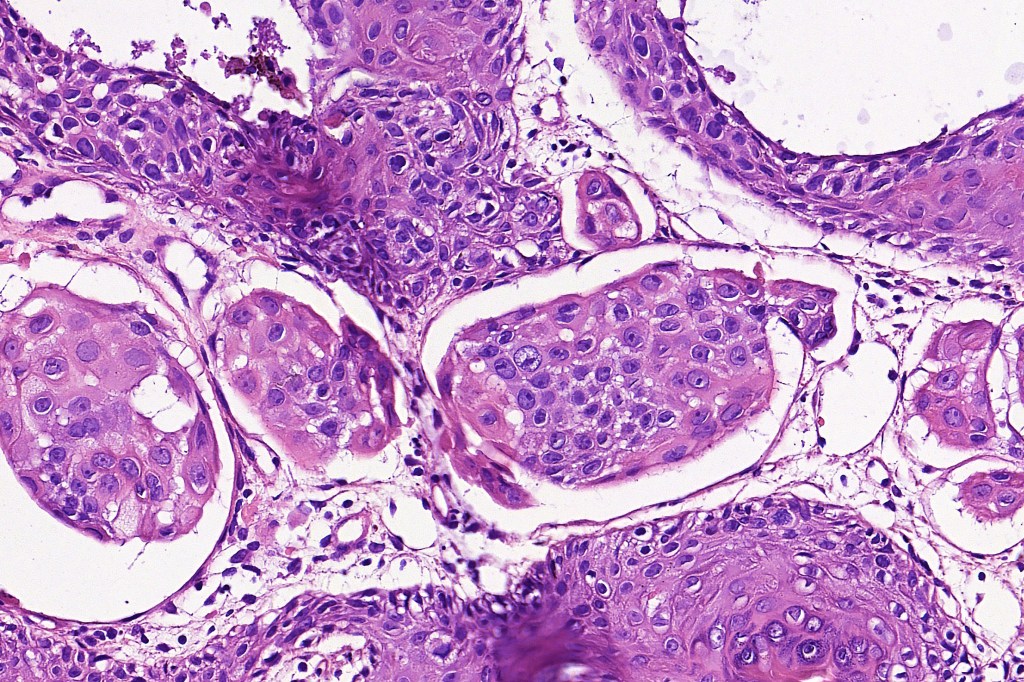
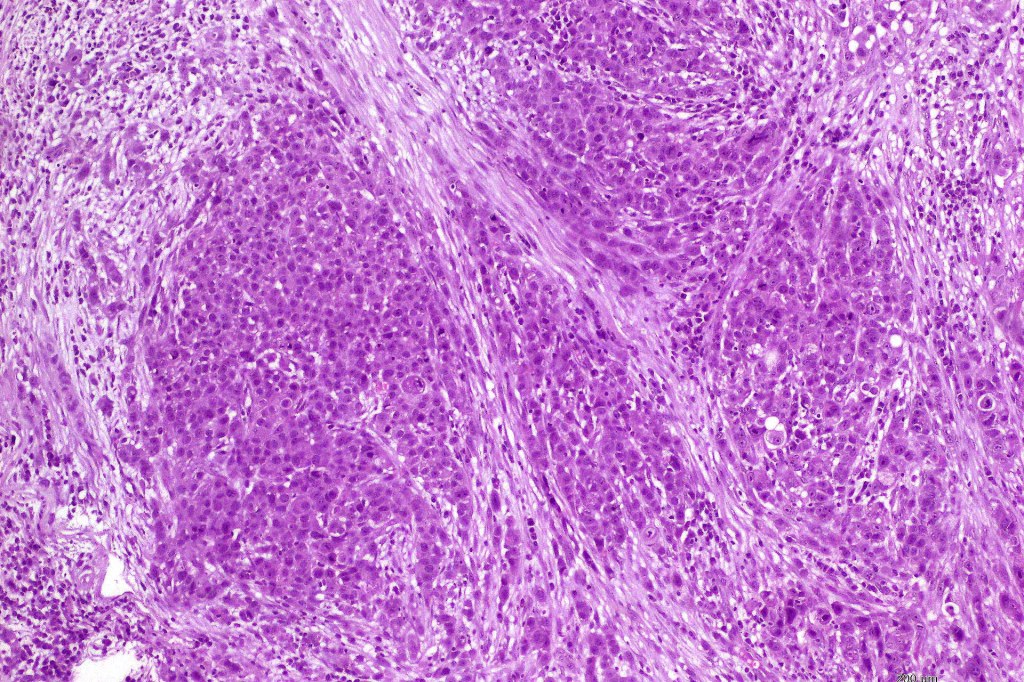
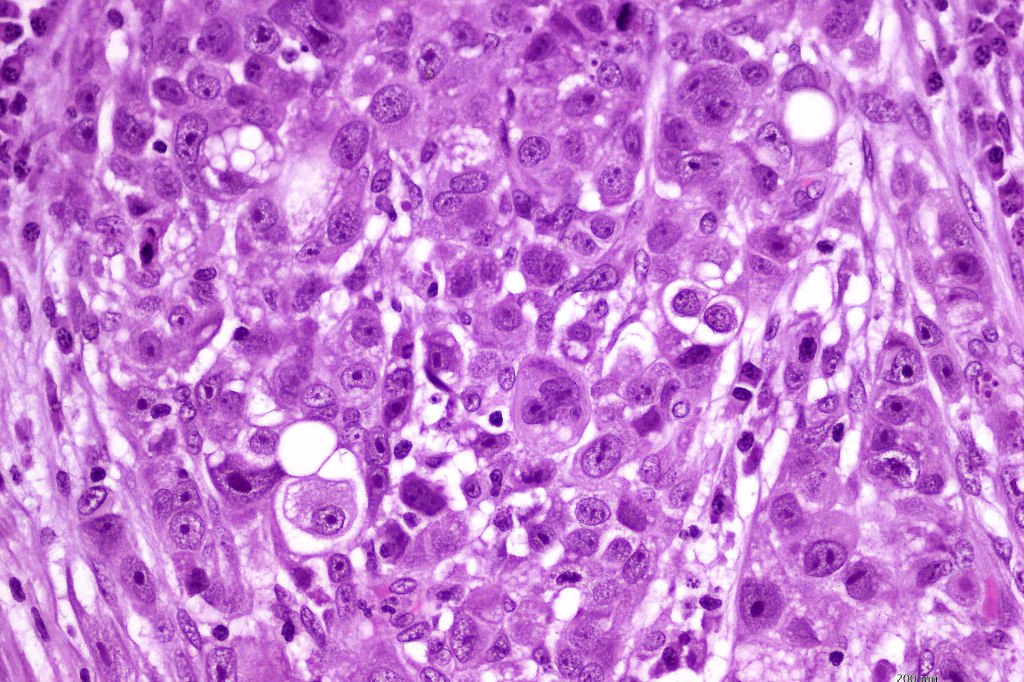
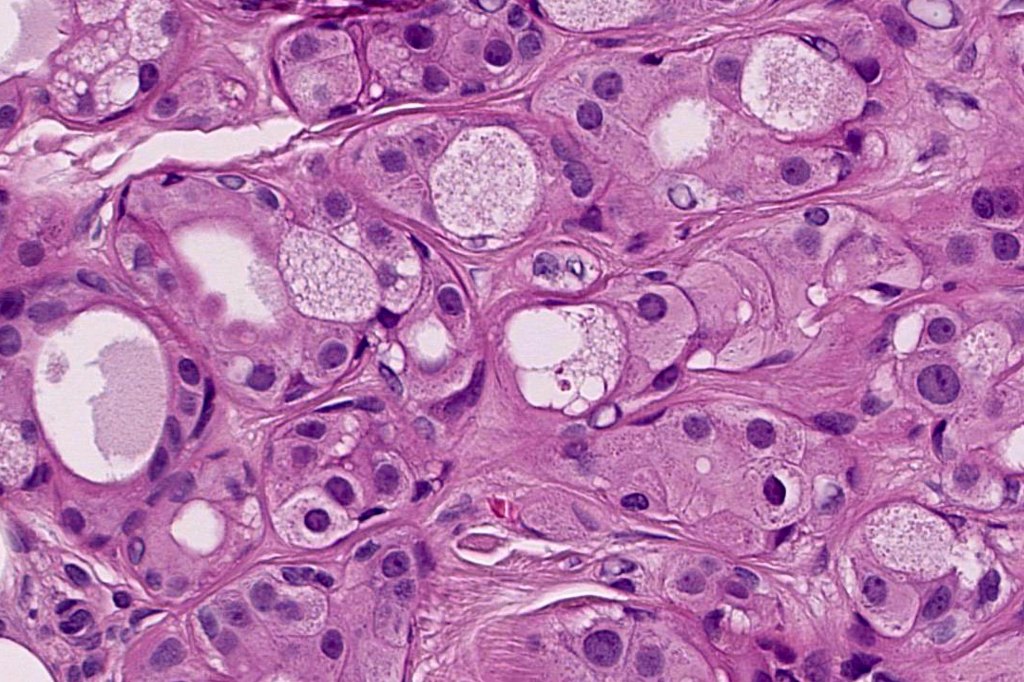
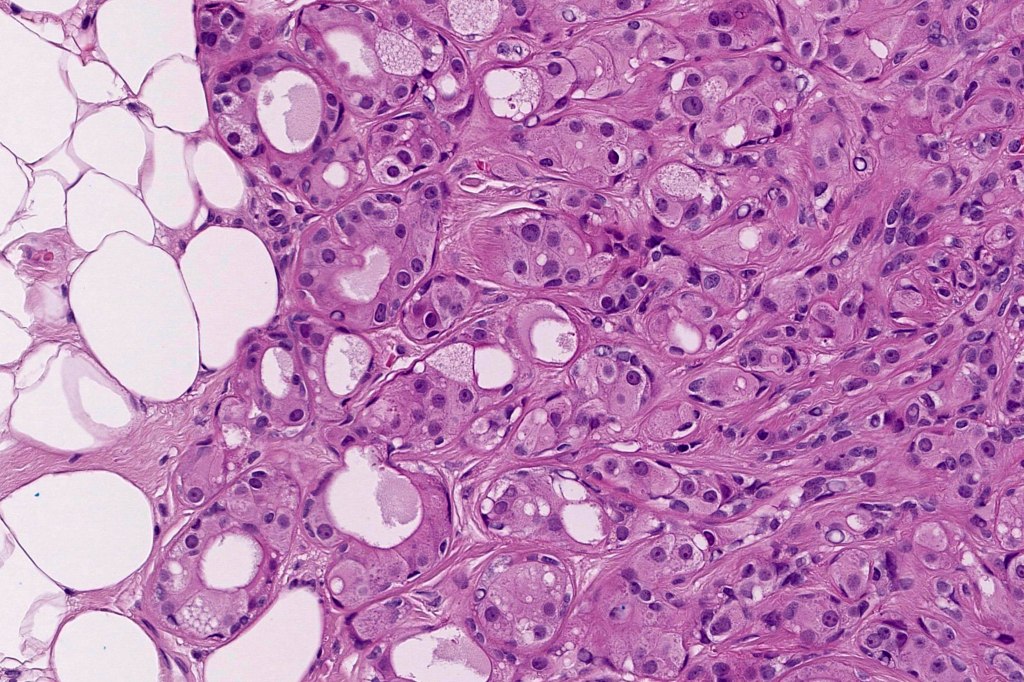
•Large cells with vesicular nuclei and often prominent nucleoli
•Decapitation secretion
•Variable pleomorphism, mitotic activity & atypical mitoses
•Variable necrosis
•Variable lymphovascular involvement & perineural infiltration
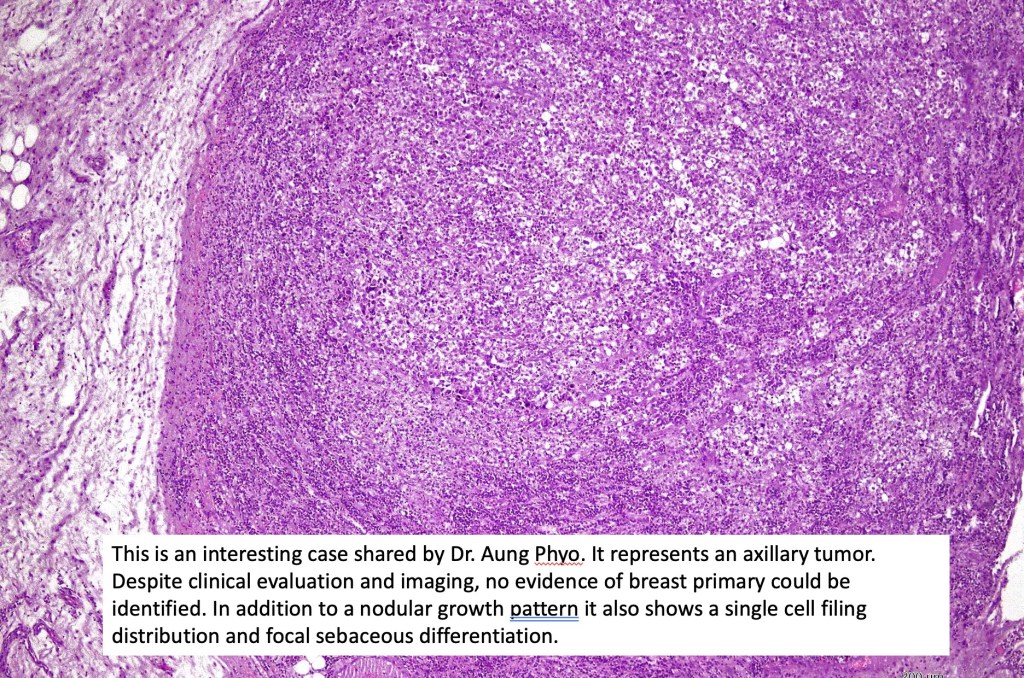
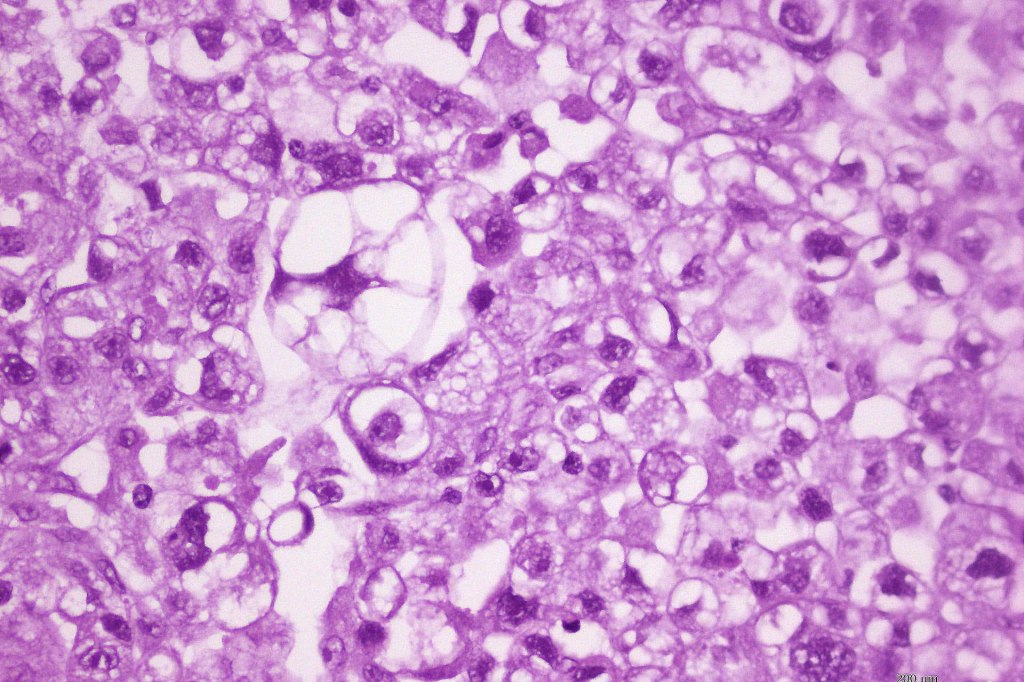
•Exceptionally squamous, clear cell, granular cell and sebaceous differentiation
•Exceptionally single file and signet ring growth pattern (see signet ring cell carcinoma)
•Intracytoplasmic DPAS +ve granules
•? Grade as per the modified Blook Richardson classification (I-3)






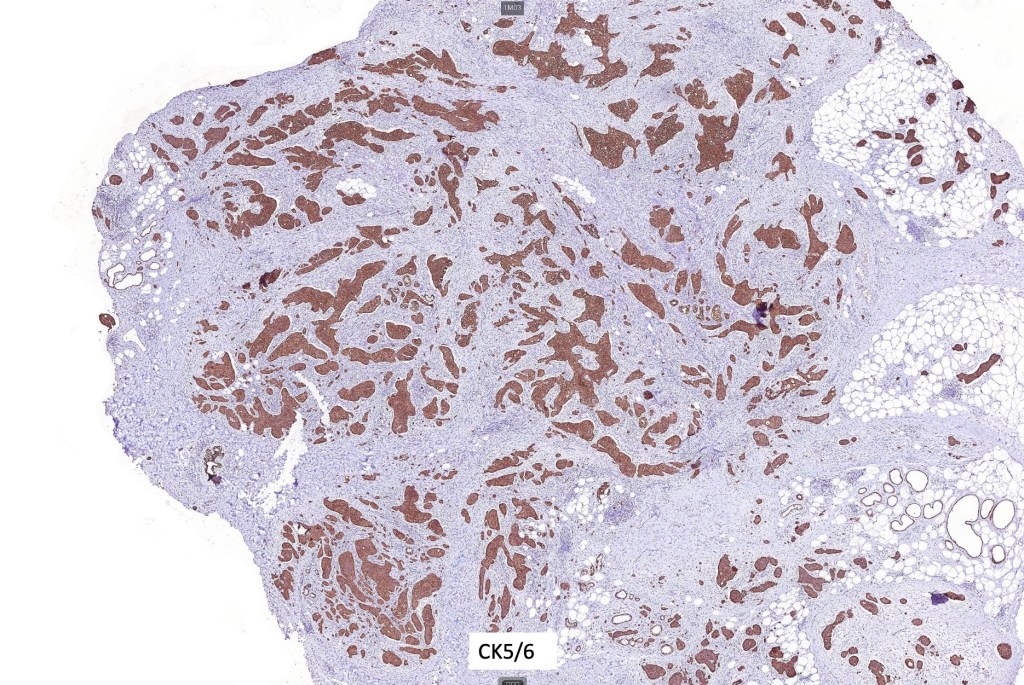
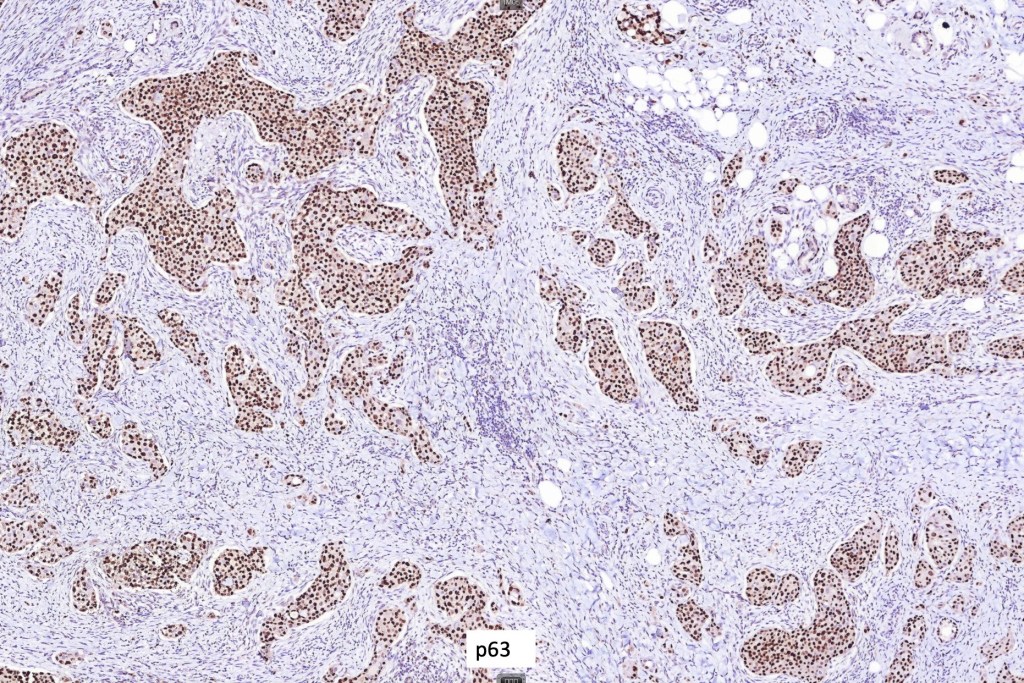
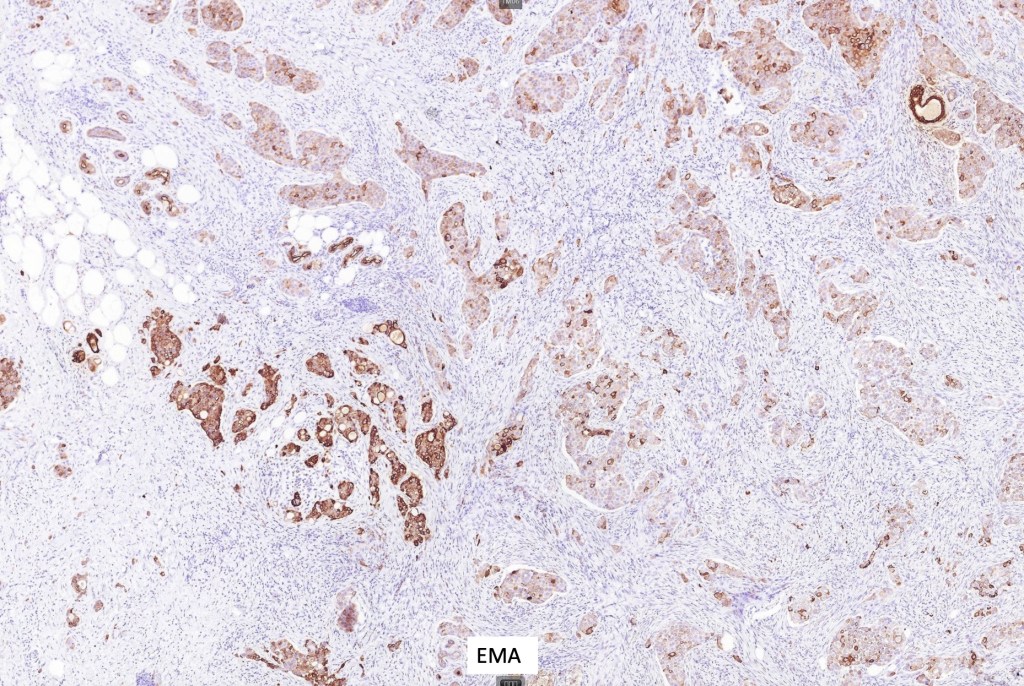
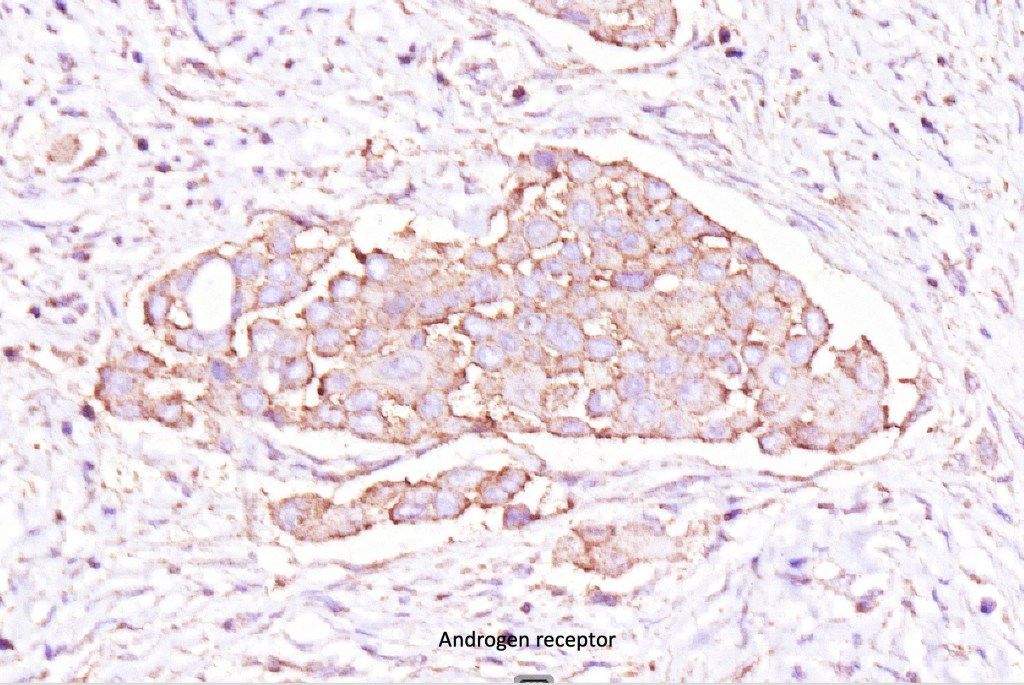
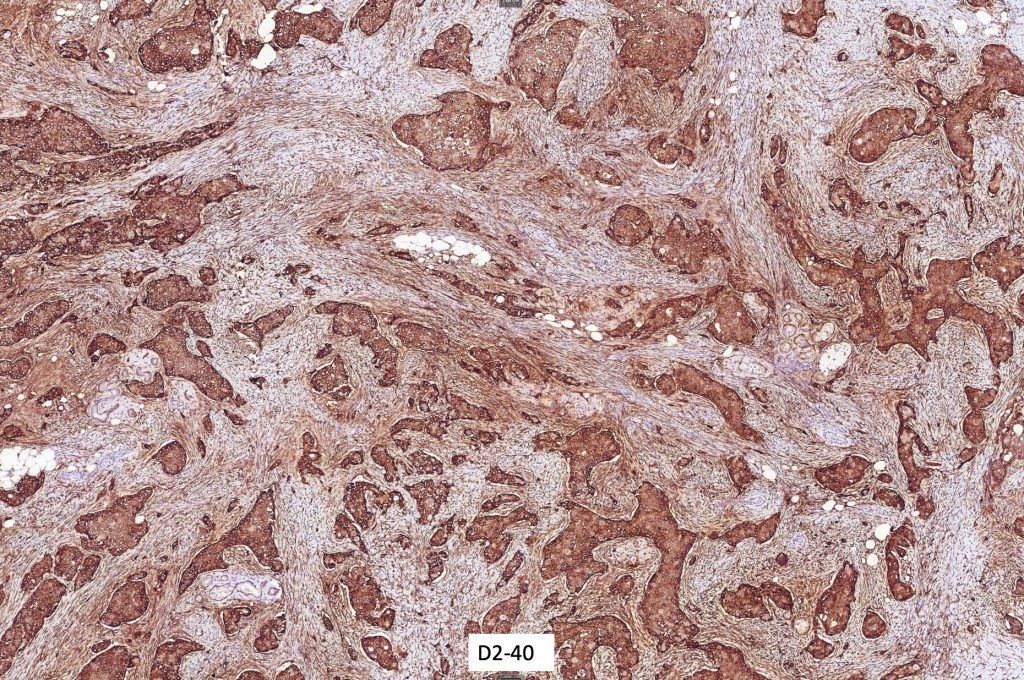
Immunohistochemistry (all images are courtesy of Dr. Kalmykova except for CK7 which was shared by Dr. Phyo)
•CAM 5.2, AE1/AE3, CK5/6, EMA, CEA, GATA3, androgen receptor, GCDFP15 and D2-40 positive
•Variable S100, SMA and p63 expression
•Variable estrogen and progesterone expression
•Adipophilin & HER2/neu negative






Differential diagnosis
Cutaneous apocrine carcinoma must always be distinguished from a breast primary tumor. Some immunohistochemical guidelines are shown in the table below.

Thank you for this helpful link! I think it’s important to say that while most breast carcinomas are ER+/PR+/AR- (hence this IHC panel is generally helpful in the distinction) breast apocrine carcinoma is characteristically triple negative (ER-/PR-/HER2-) and AR+.

Leave a comment