Clinical features
•Very rare
•Solitary– elderly F>M, 1-2 mm skin-colored papule with a predilection for the face & scalp but may occur elsewhere
•Localized– pink or brown plaque with a predilection for scalp, +/- milia & alopecia
•Linear nevoid– congenital/acquired, dermatomal, can be very extensive +/- alopecia, BCC, epidermoid cysts & comedones
•Segmental– associated with osseous & dental malformations & cerebral defects
•Generalized– facial plaques, alopecia totalis +/- myasthenia gravis, cystic fibrosis, thyroid abnormalities, hyperhidrosis & SLE
•Generalized may also be associated with tuberous sclerosis, Cowden-, Gorlin-Golz- & Rombo syndromes
•Autosomal dominant inherited variant- childhood & adult forms
Histological features
•Mutation in PTCH-1 gene (encodes receptor for protein product of Sonic Hedghog gene)
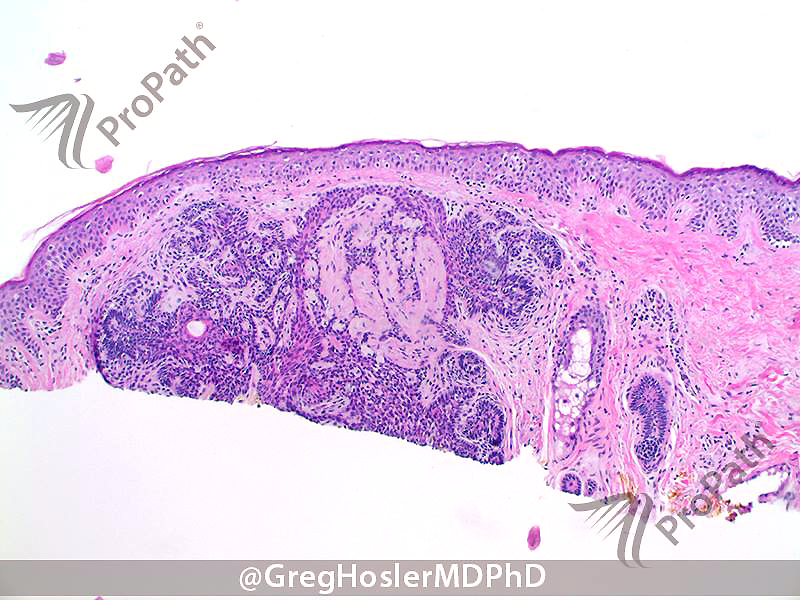
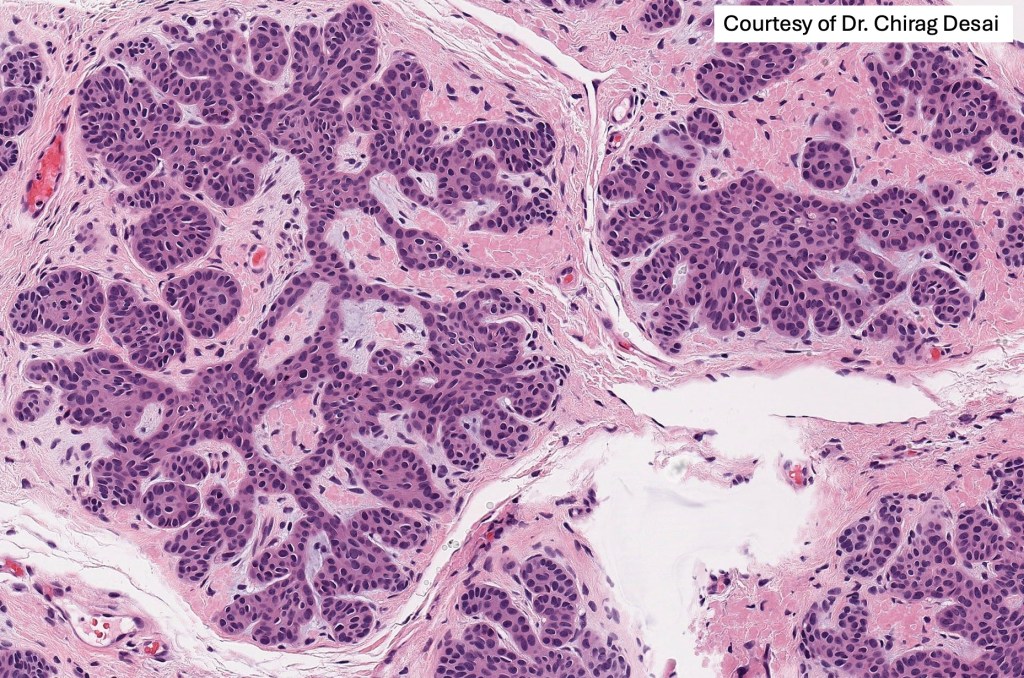
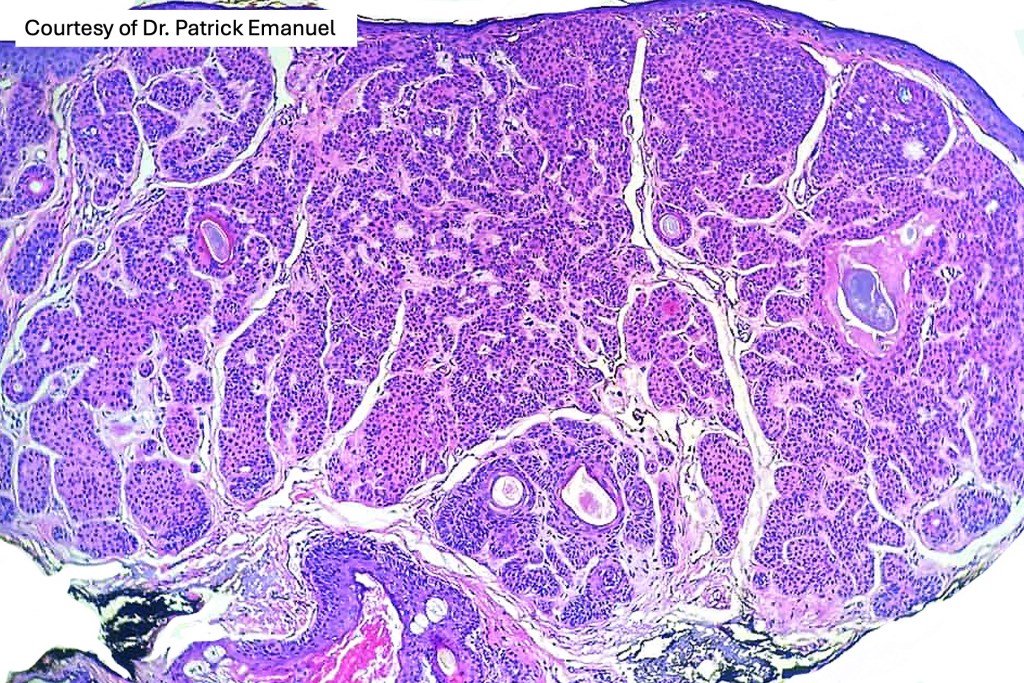
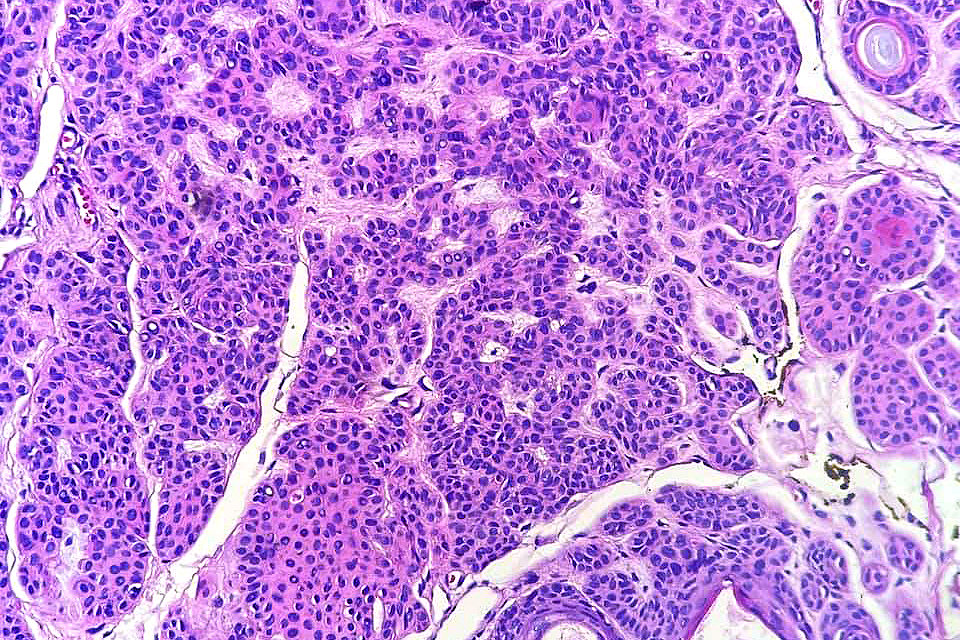
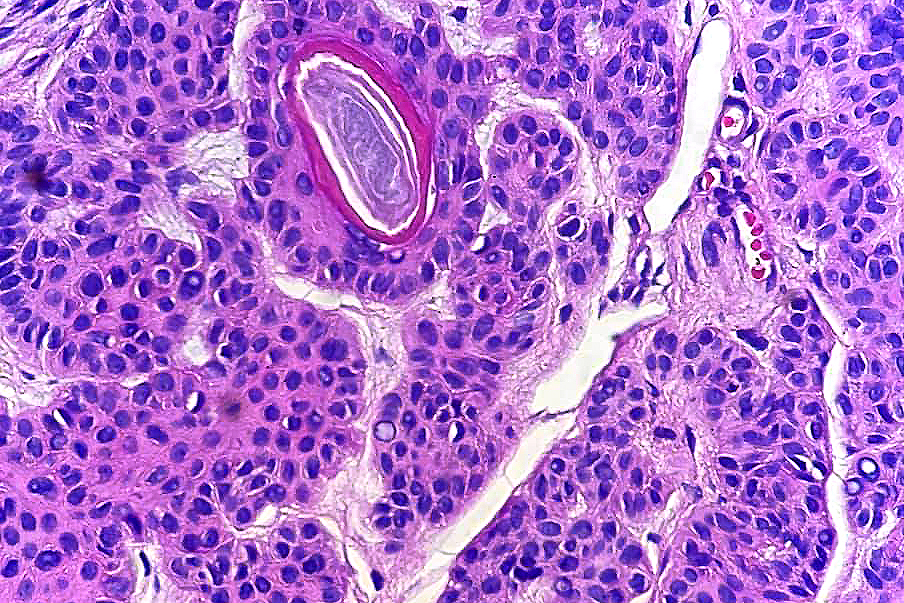
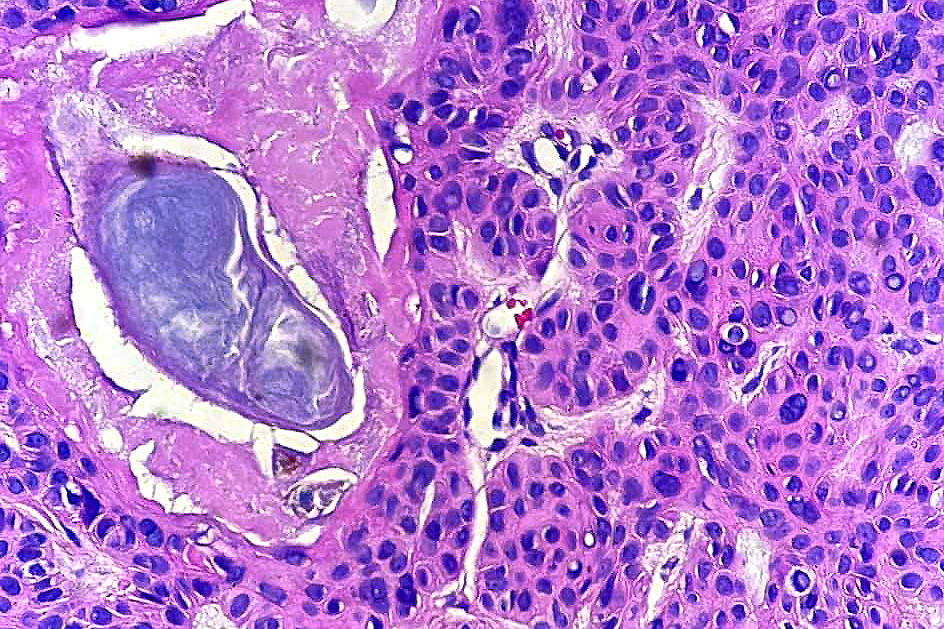
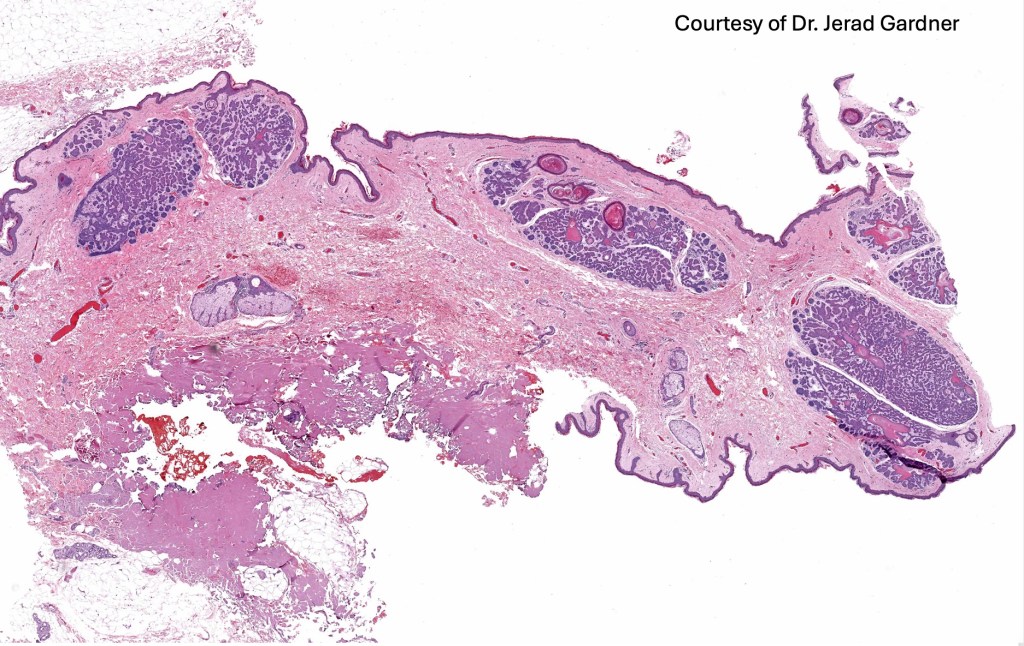
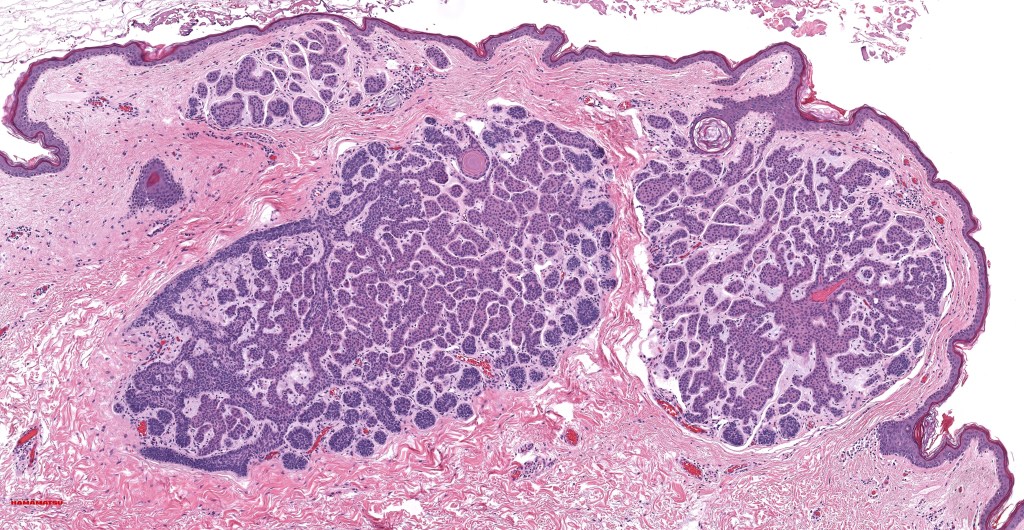
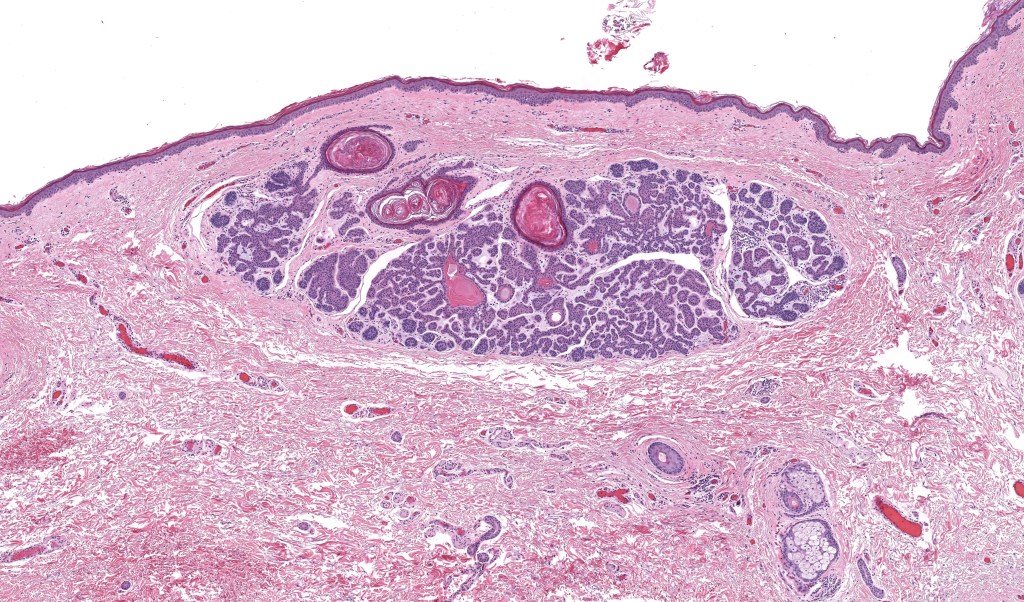
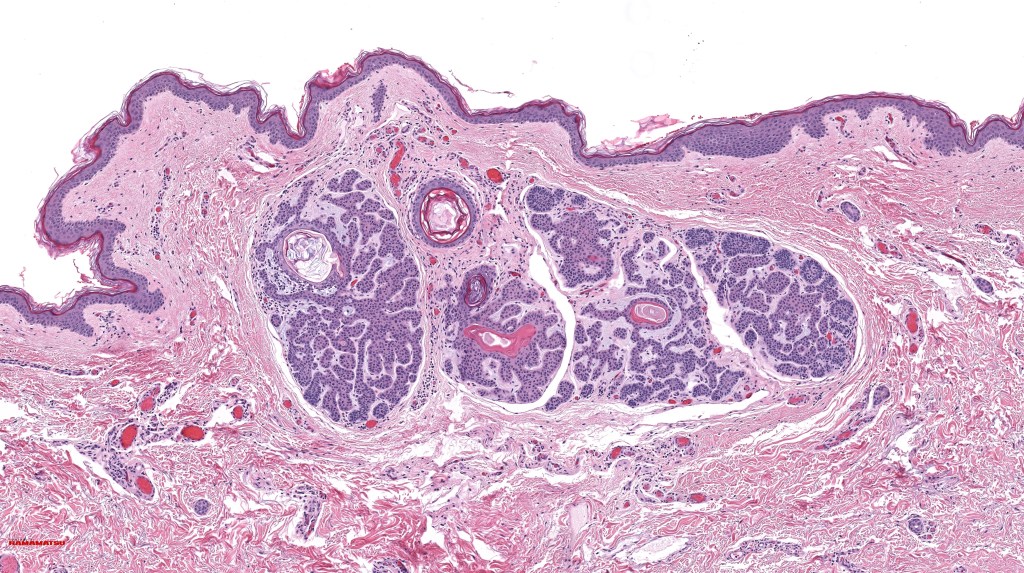
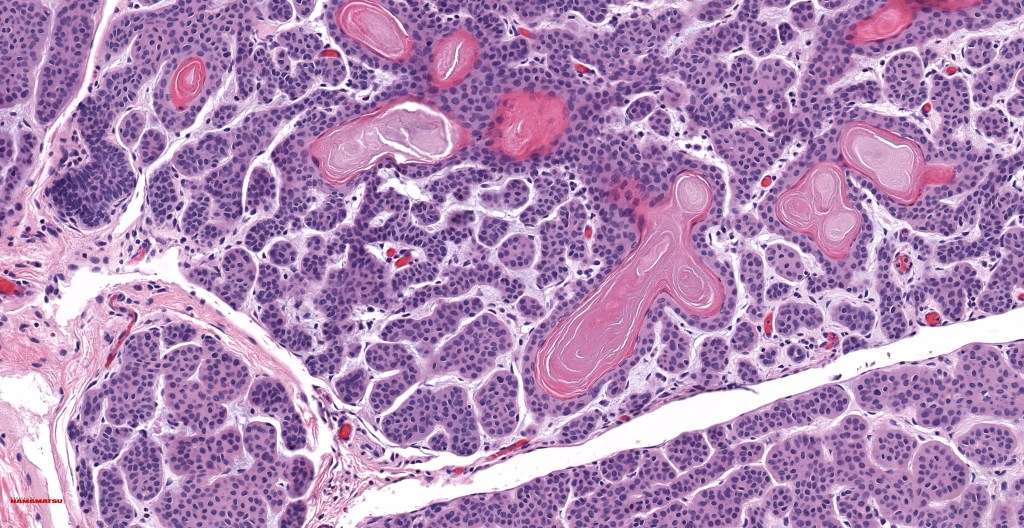
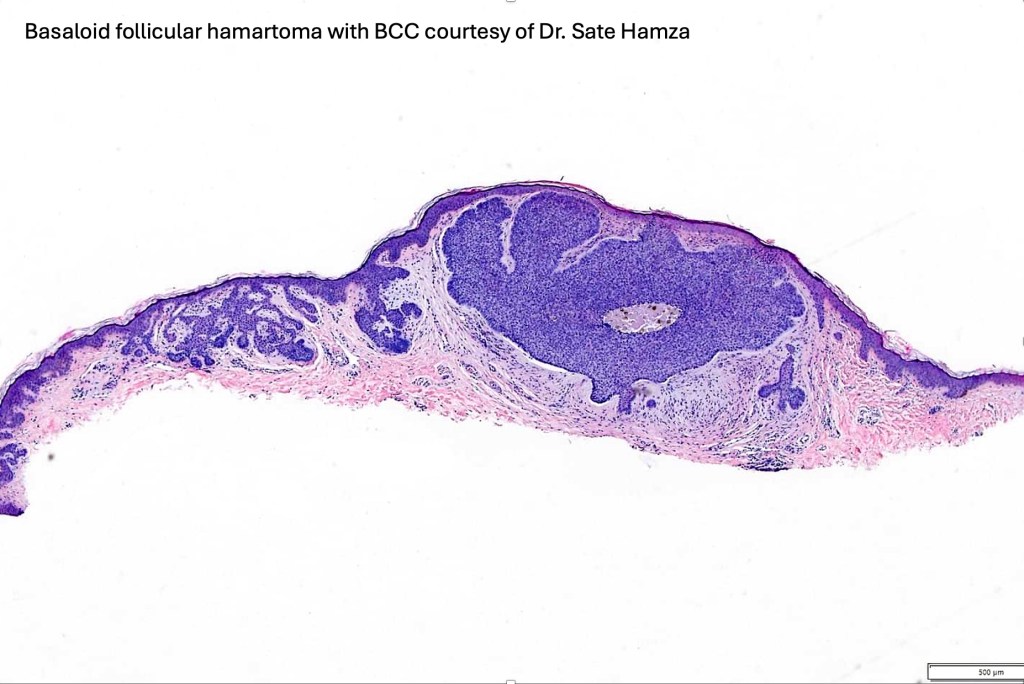
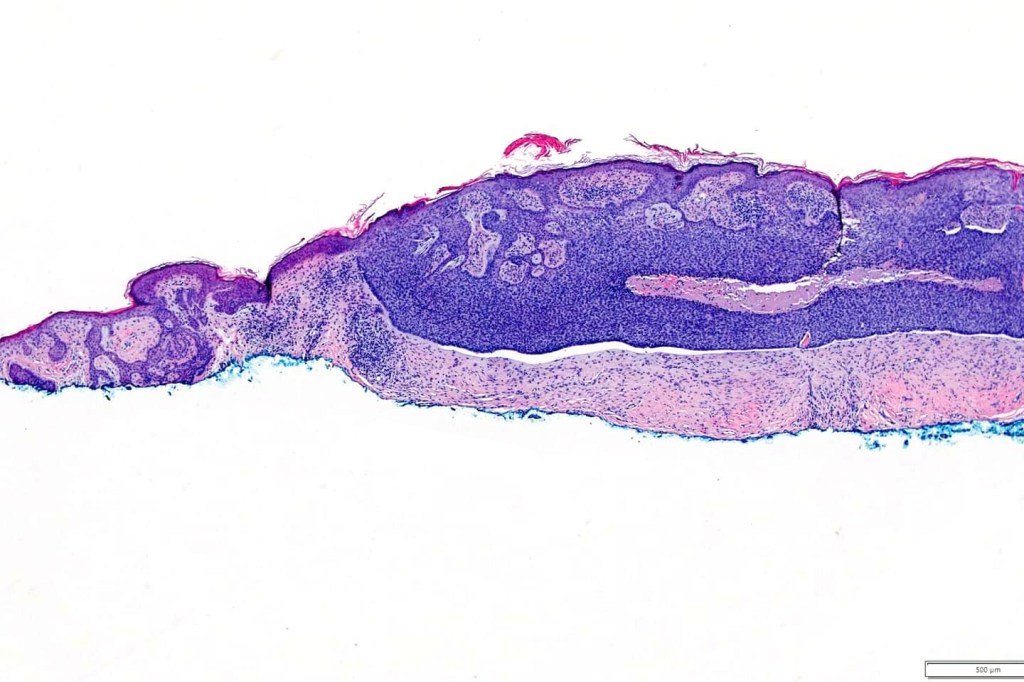
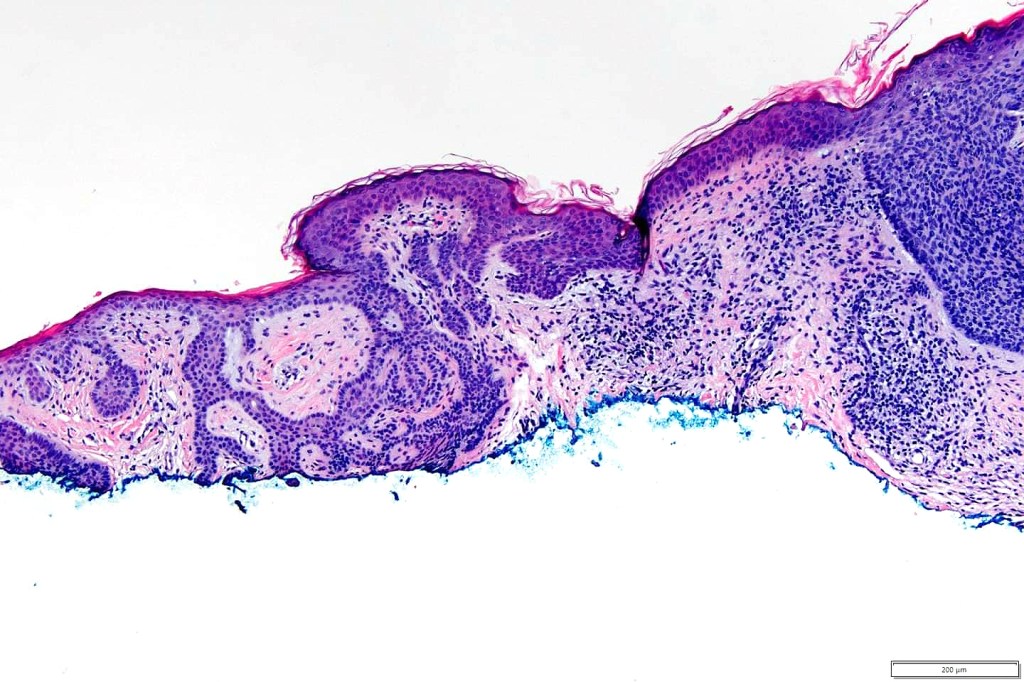
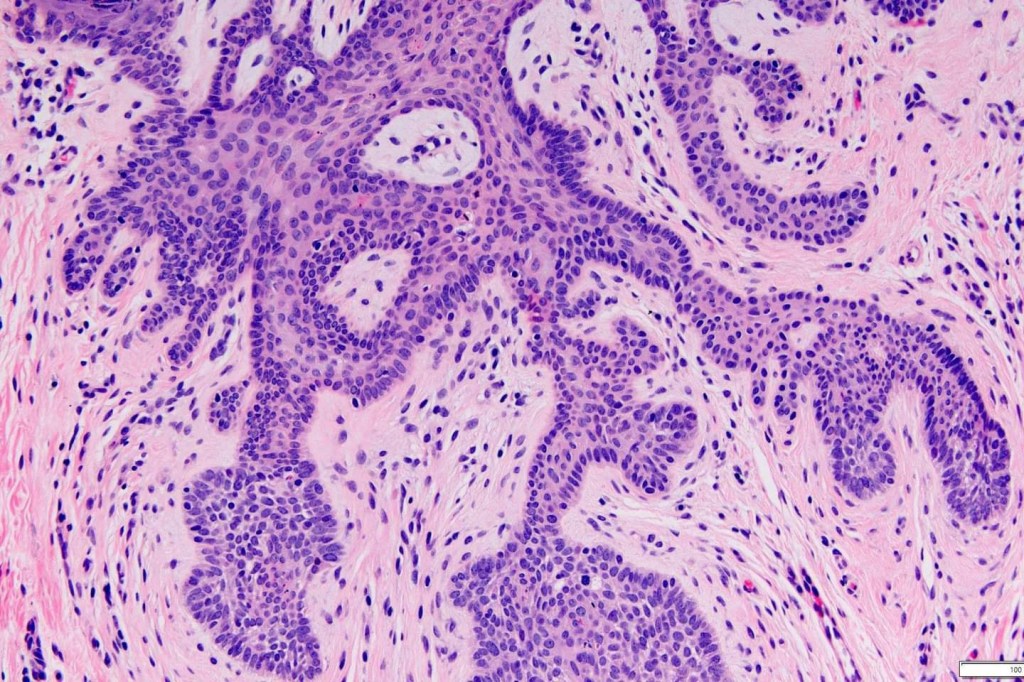
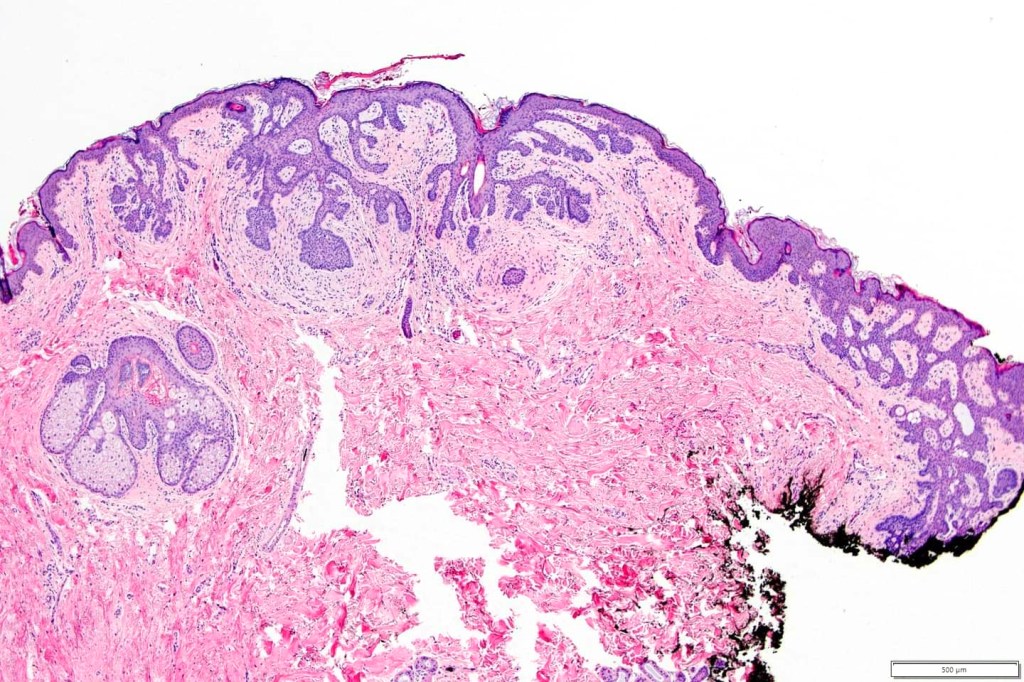
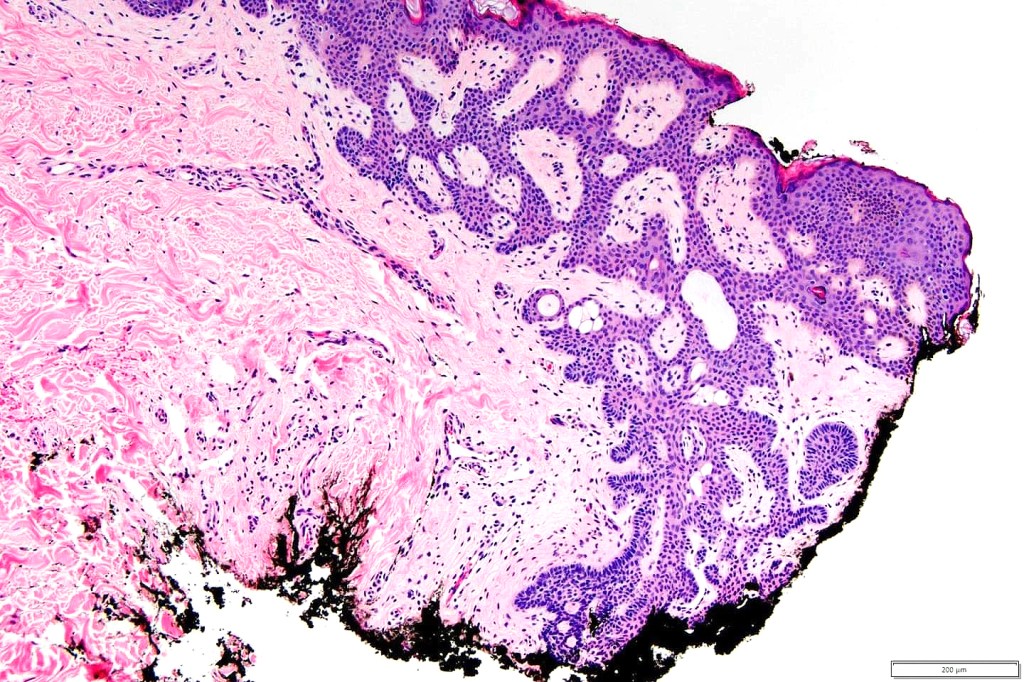
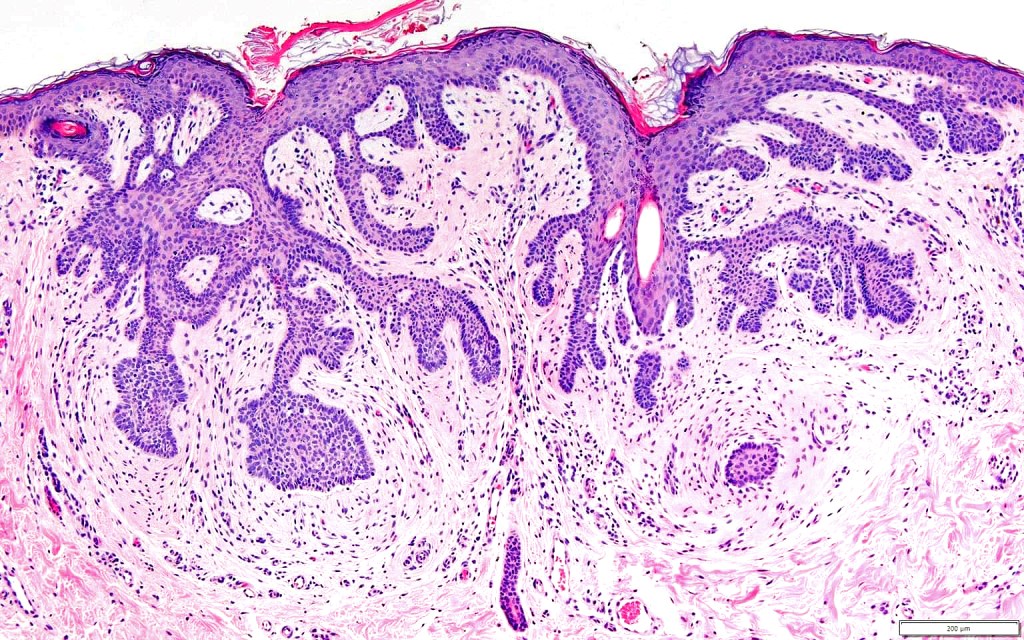
•Vertically orientated, folliculocentric, thin, anastomosing strands composed of basaloid cells embedded in a loose fibrous stroma
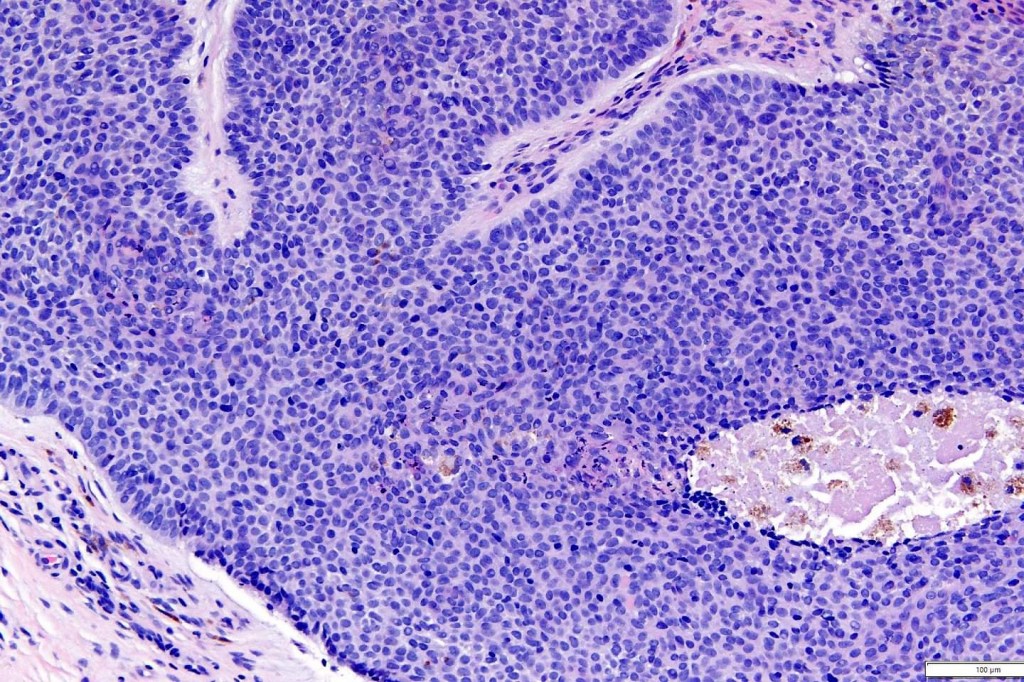
•No pleomorphism
•No mitoses
•Epidermal origin sometimes evident
•+/- peripheral palisading
•Variable keratocysts
•No retraction artifact or stromal mucin deposition
•Sometimes, in addition, trichoepithelioma-like lesions are present
•BCC may complicate, particularly in the linear nevoid variant
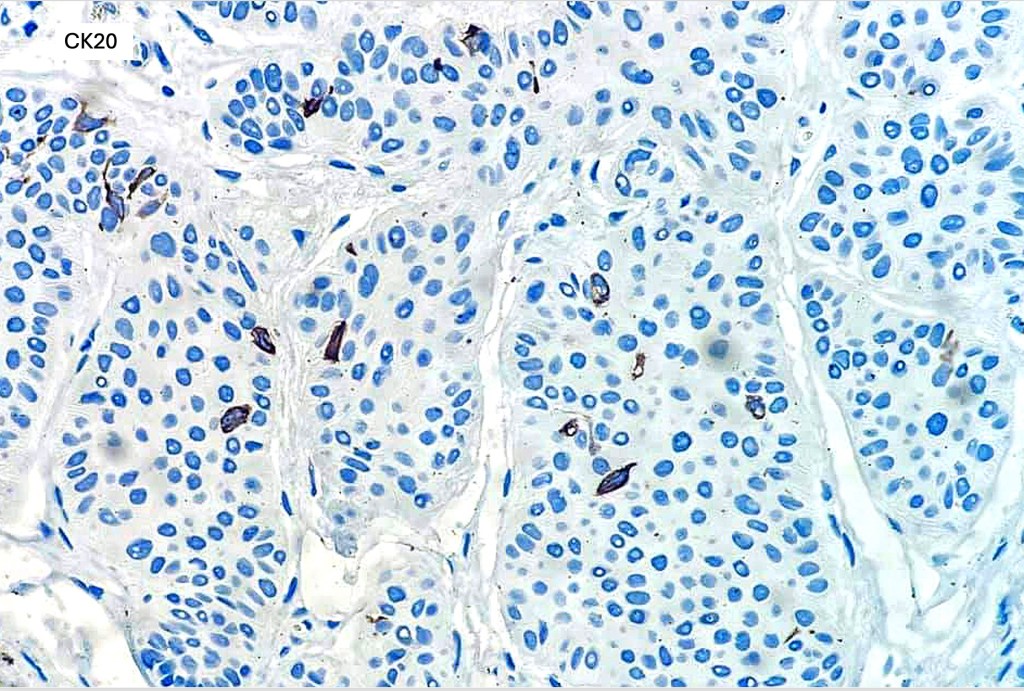
•CD20+ve Merkel cells
•Stromal CD34 +ve cells
•Outermost layer bcl-2 expression (compare with BCC)
•Low Ki67 expression (compare with marked expression in BCC)

Differential diagnosis
In the majority of cases, the diagnosis is straighforward. In case of any difficulty, basaloid follicular hamartoma can be distinguished from basal cell carcinoma by the absence of nodules, retraction artifact and stromal mucin deposition. The immunohistochemistry profile is quite different (see histology).

Leave a comment