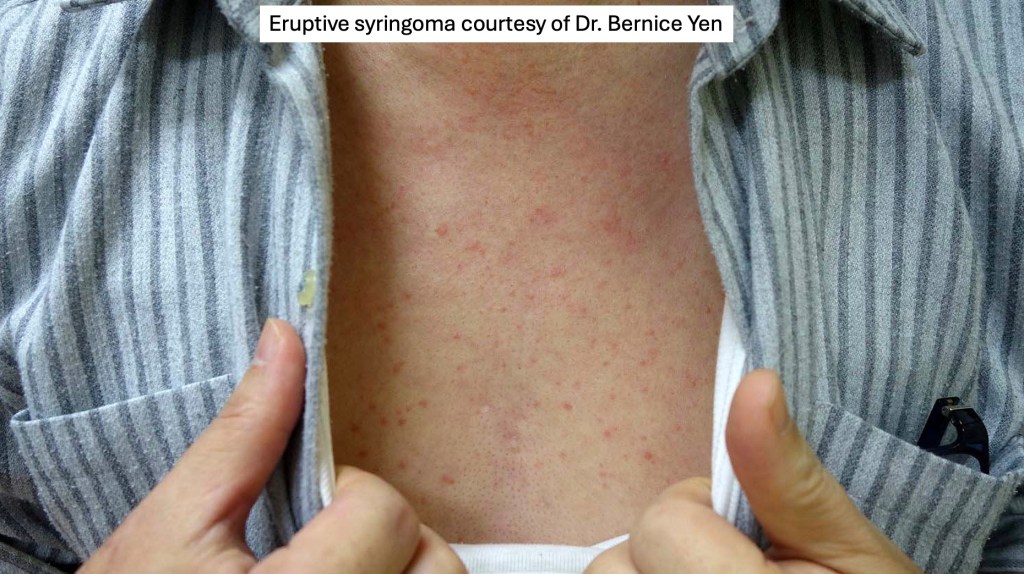
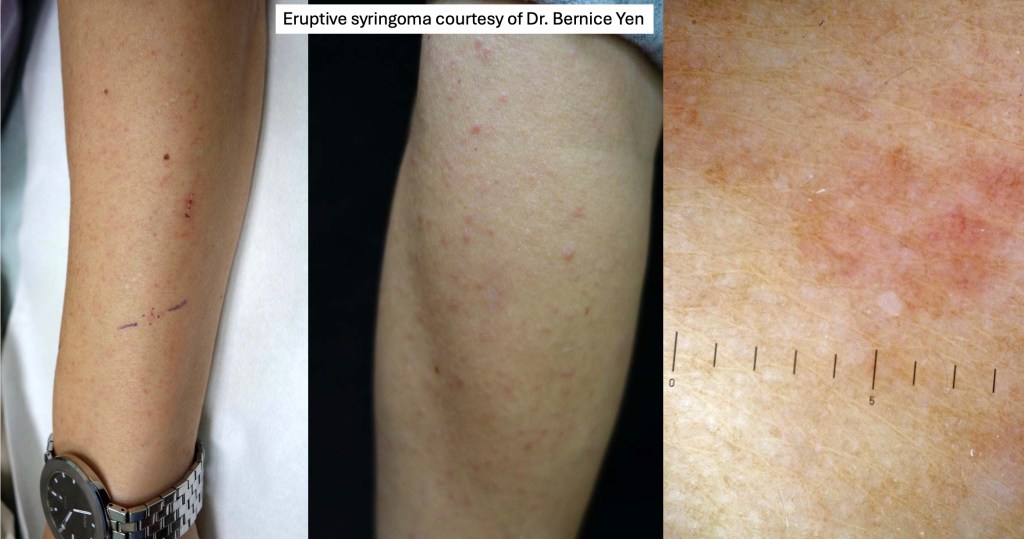
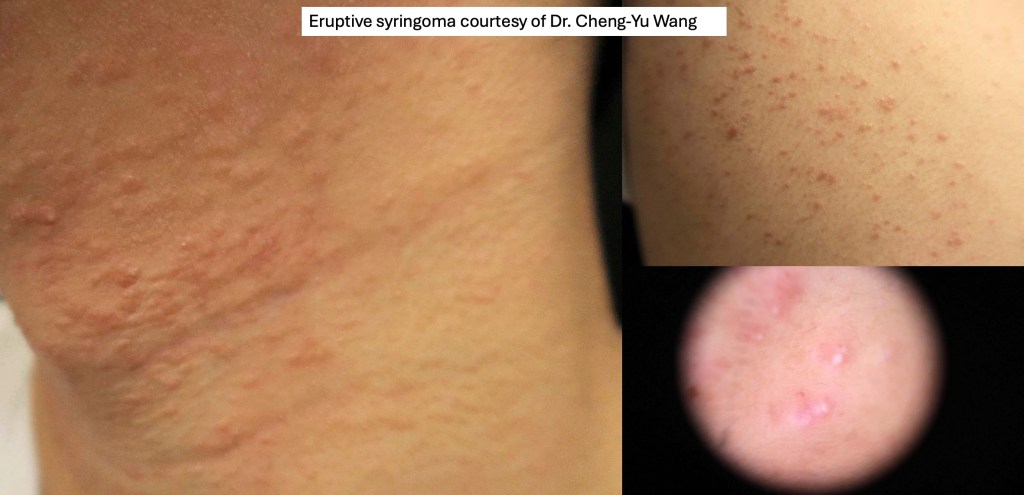
Clinical features
•Commonly present on the lower eyelids & upper cheeks as multiple flesh colored or yellow/brown small (1-3 mm) papules; although they can present just about anywhere
•Vulval syringomas are often associated with marked pruritus
•F>>M
•Teenagers & young adults
•May be familial, autosomal dominant (16q22)
•Increased incidence in Asian females
•Unilateral linear nevoid following Blaschko’s lines
•Plaque variant (may mimic microcystic adnexal carcinoma)
•Associations with Down’s-, Brooke-Spiegler- & Ehlers-Danlos syndromes

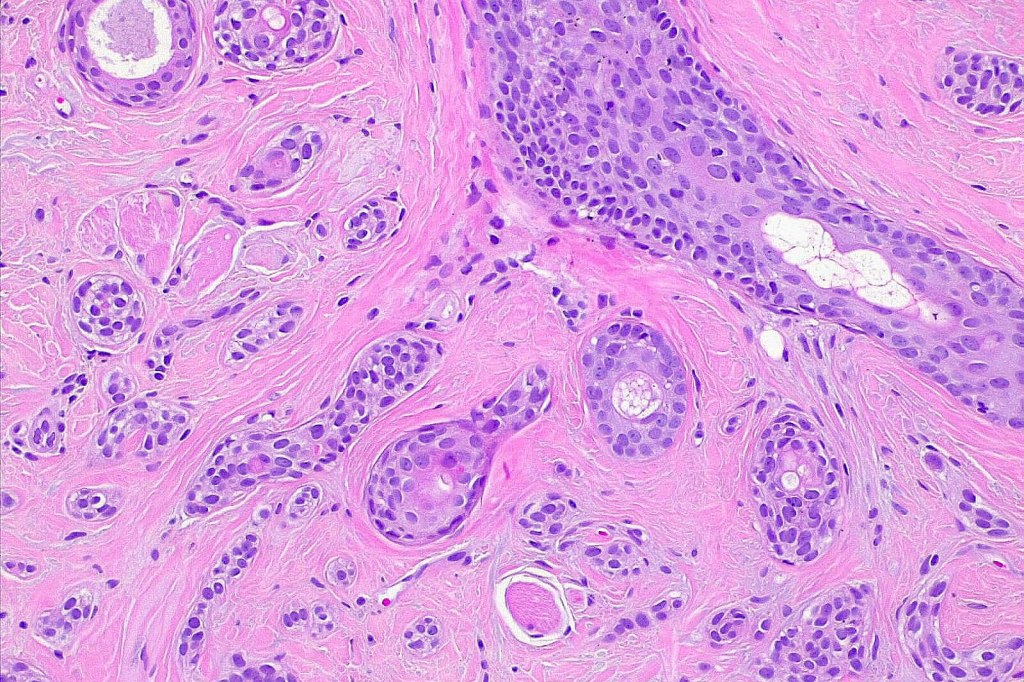
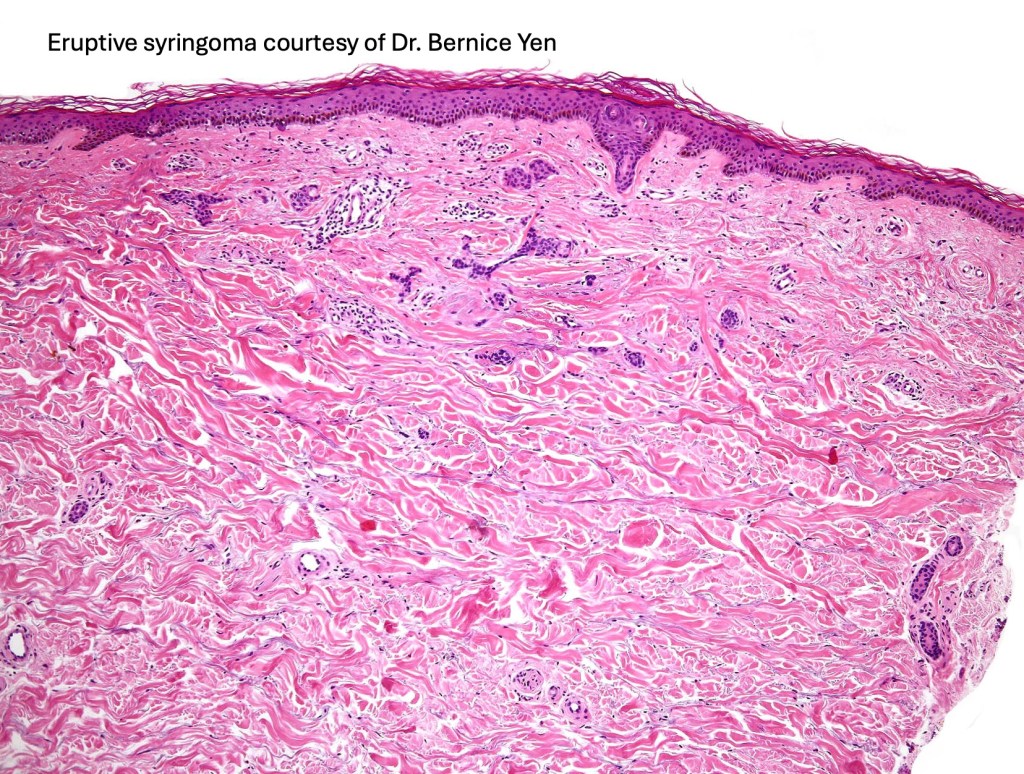
Histological features
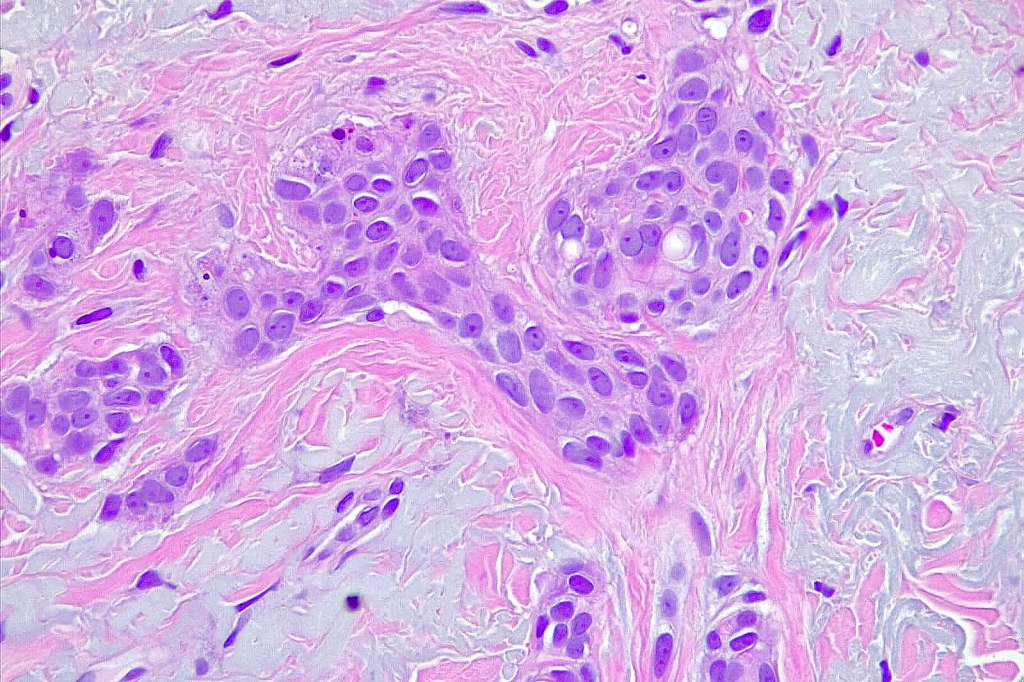
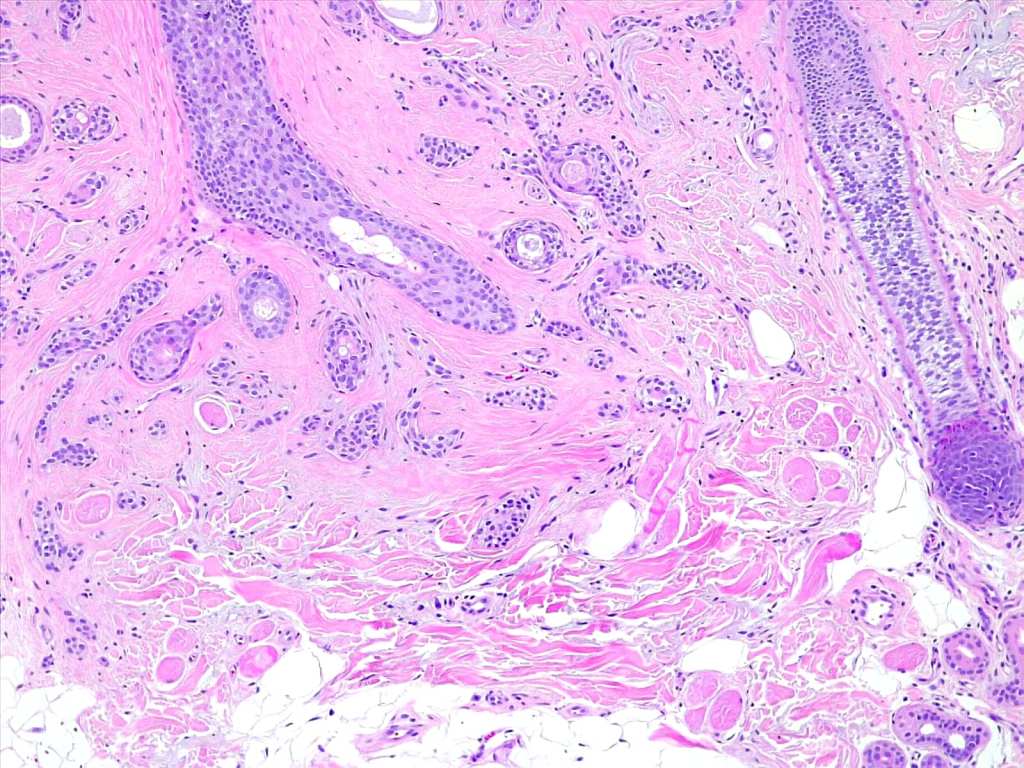
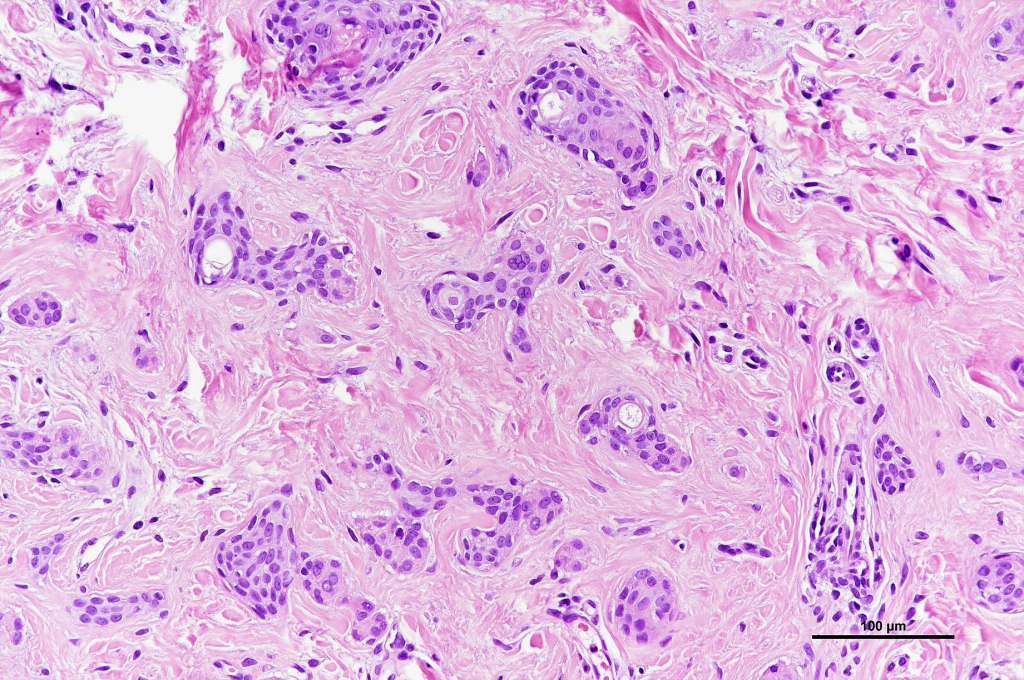
•Dermal lesion composed of epithelial stands & ducts dispersed in a fibrous stroma
•Tadpole configuration- ducts with epithelial strands
Intracytoplasmic lumina
•Clear cell variant (associated with diabetes mellitus)
•Absence of pleomorphism or mitotic activity
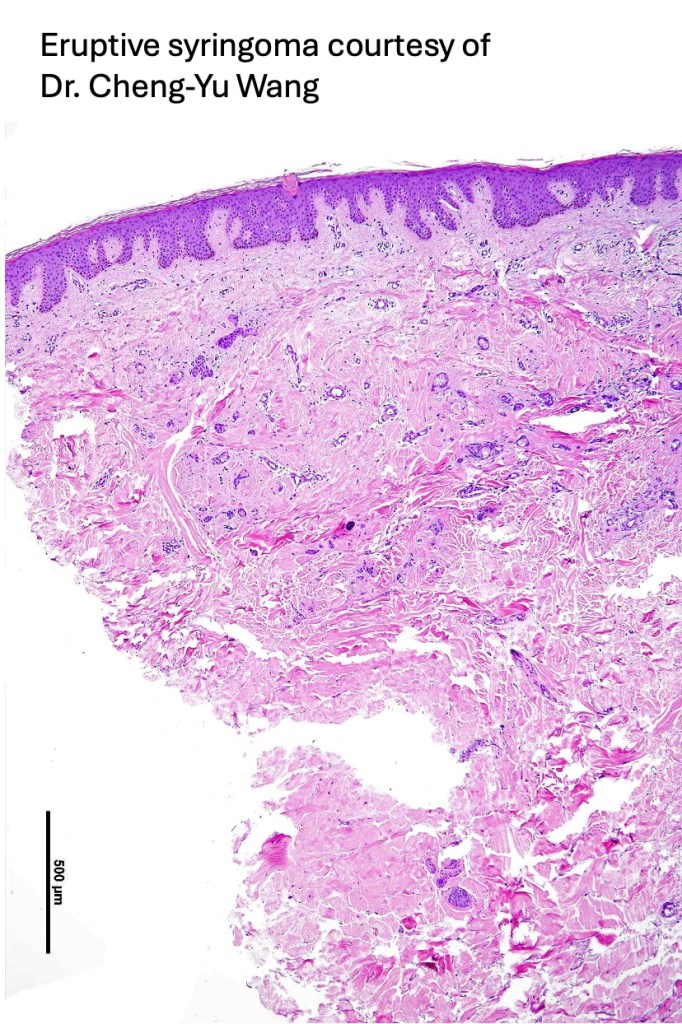
•Eruptive milium-like syringoma characterized by a superficial keratin filled cyst associated with an underlying syringoma
EMA & CEA to highlight ductal differentiation in diffiuclt cases











Differential diagnosis
Generally speaking, syringoma should not pose any diagnostic difficulties. However shave biopsies can sometimes be problematical. Syringoma differs from desmoplastic trichoepithelioma by the presence of ducts & intracytoplasmic lumina. Microcystic adnexal carcinoma can be distinguished by the presence of keratocysts in the superficial component. In addition, the clinical appearance is quite difference.

Leave a comment