Clinical features
•Very poor prognosis
•Exceptionally rare & is only seen in stage IV disease (I have only seen three cases in 52 years!)
•Bimodal age distribution for Hodgkin lymphoma- teenagers & over 50’s
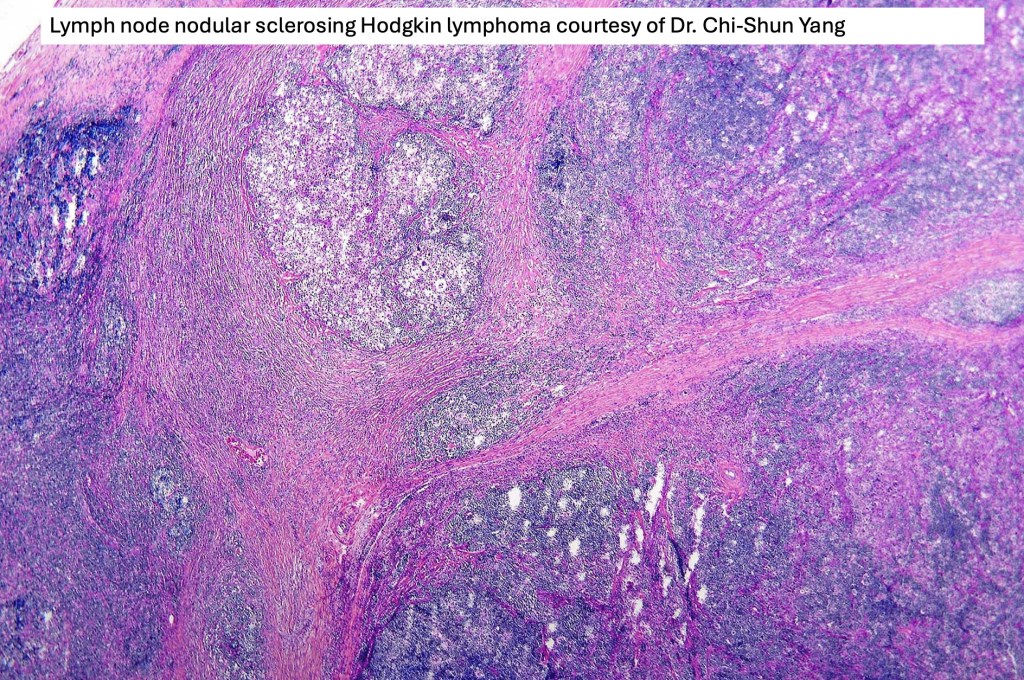
•Nodular sclerosis>mixed cellularity>lymphocyte depleted
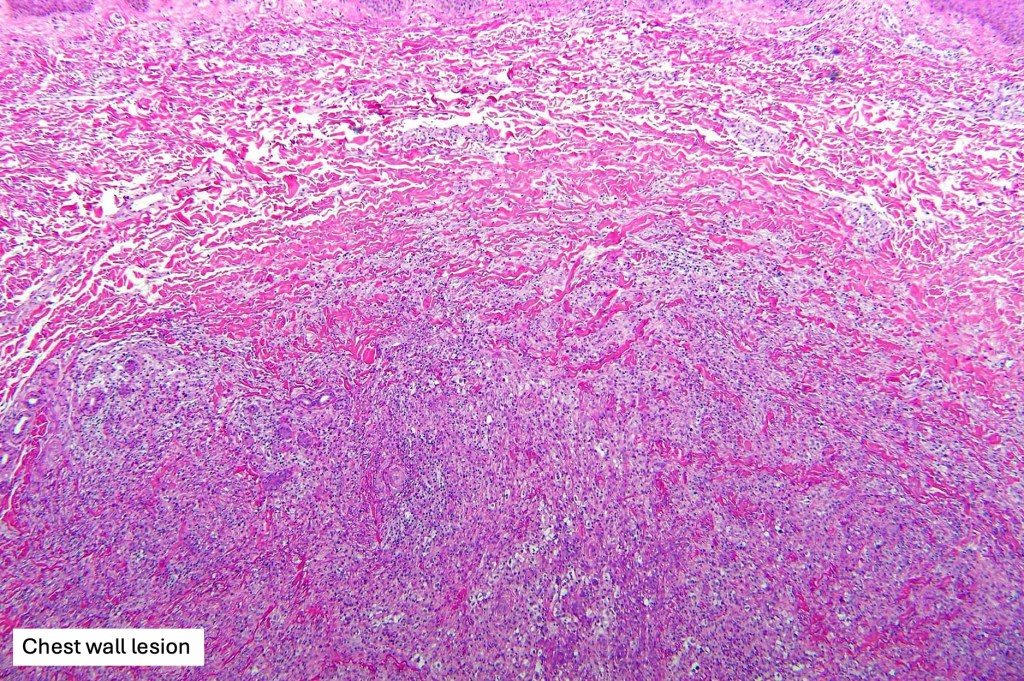
•Nodal disease extending to the skin, retrograde lymphatic spread andmetastatic disease
•Single or multiple pink to red papules, nodules & plaques
•Chest, head & neck, inguinal region, axilla but can present anywhere
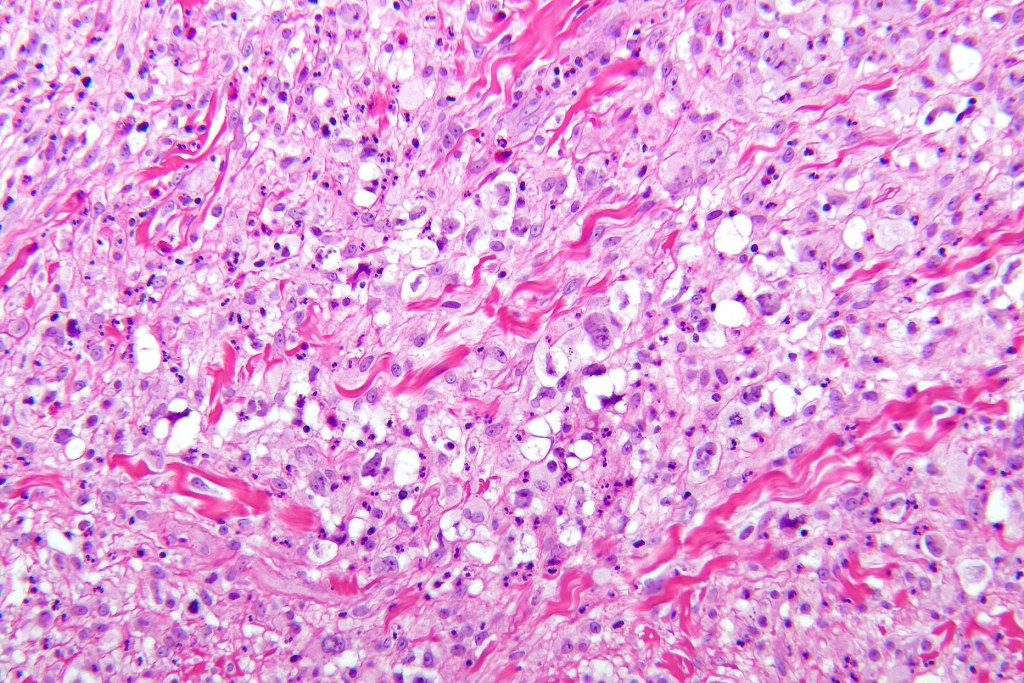
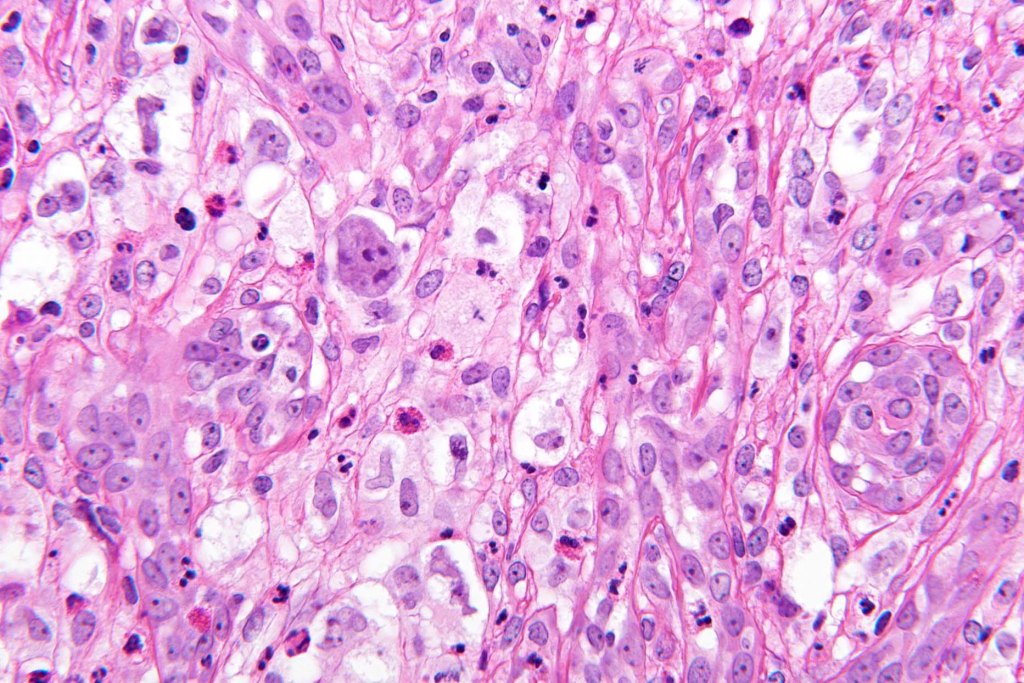
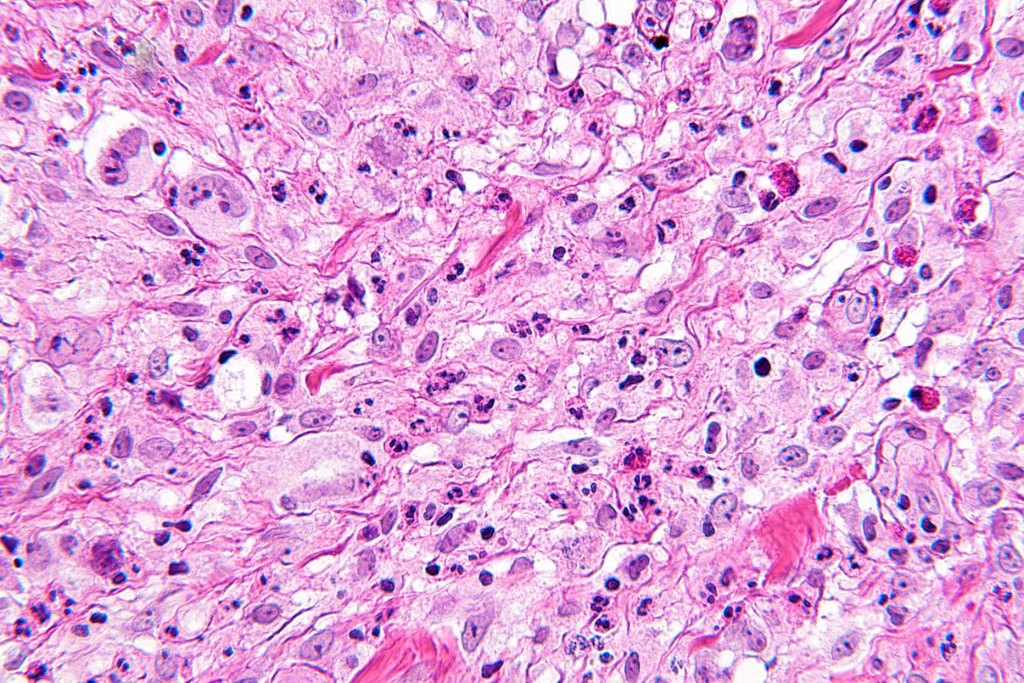
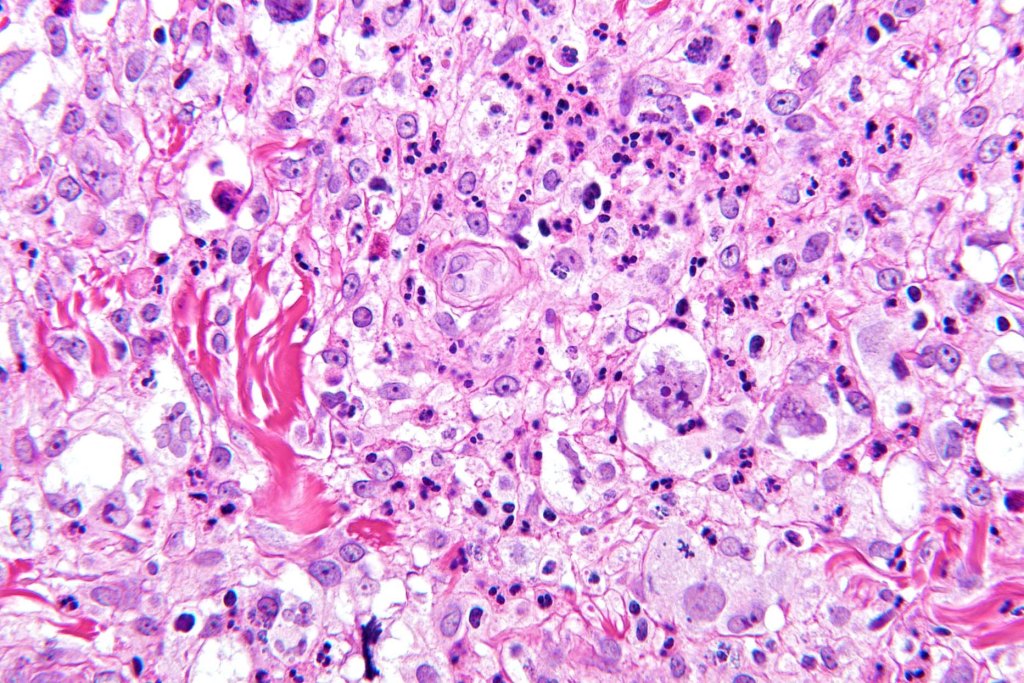
Histological features
•Hodgkin lymphoma- association with EBV, HIV & infectious mononucleosis
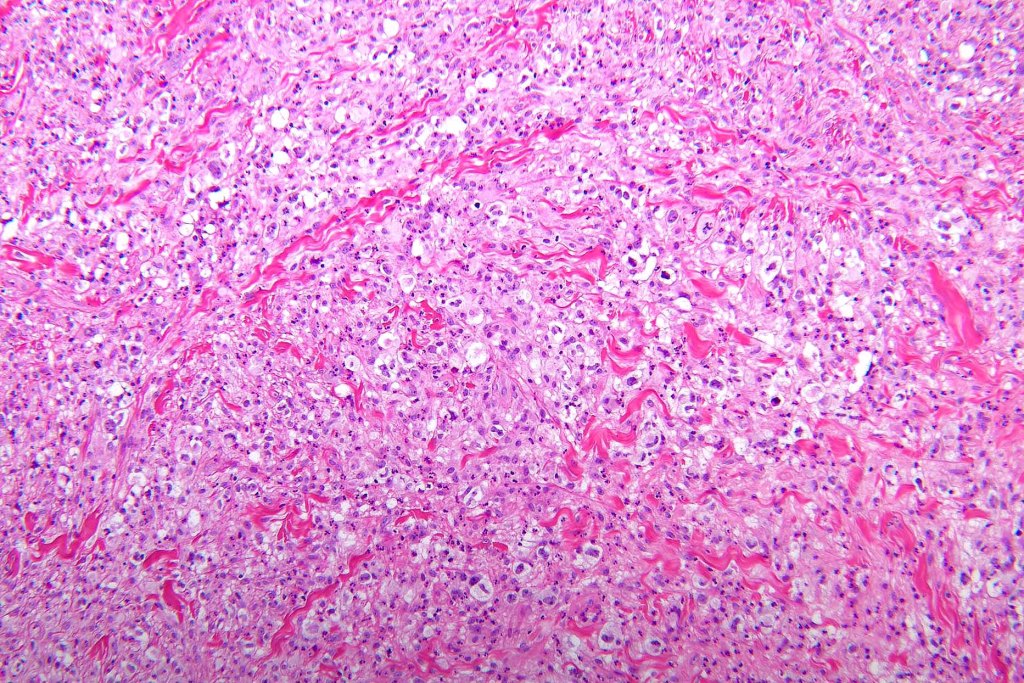
•Diffuse or nodular infiltrate, sometimes with ulceration
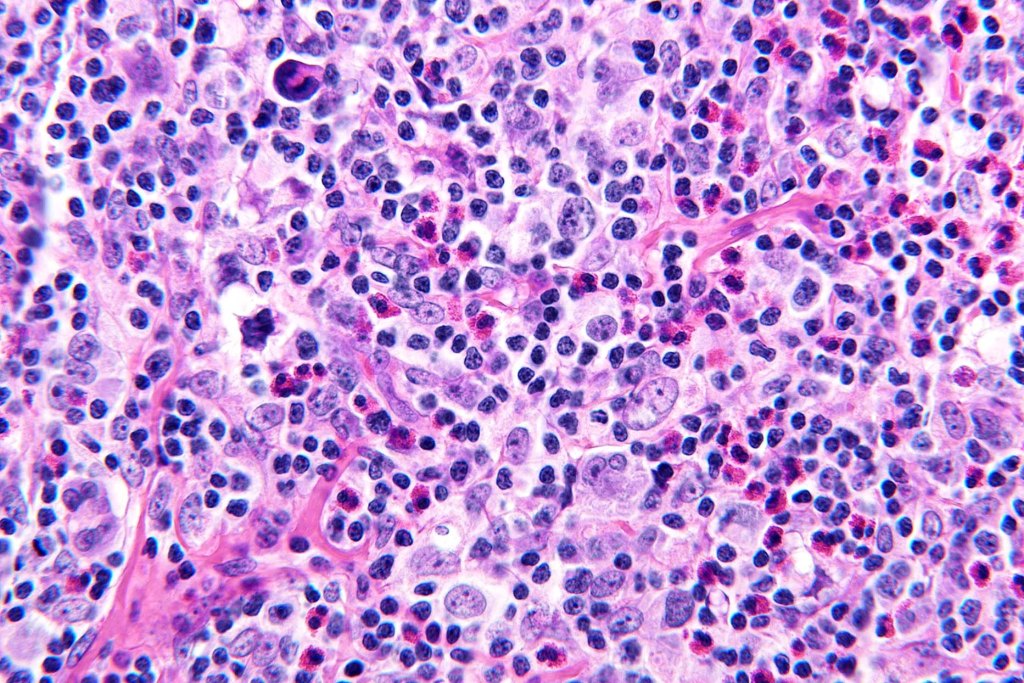
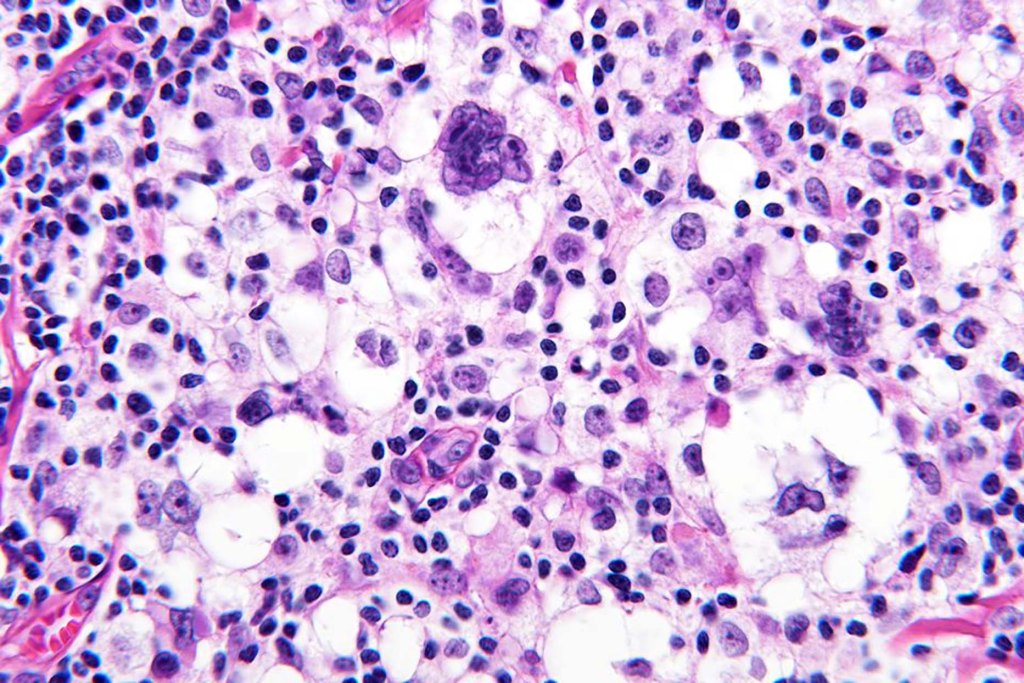
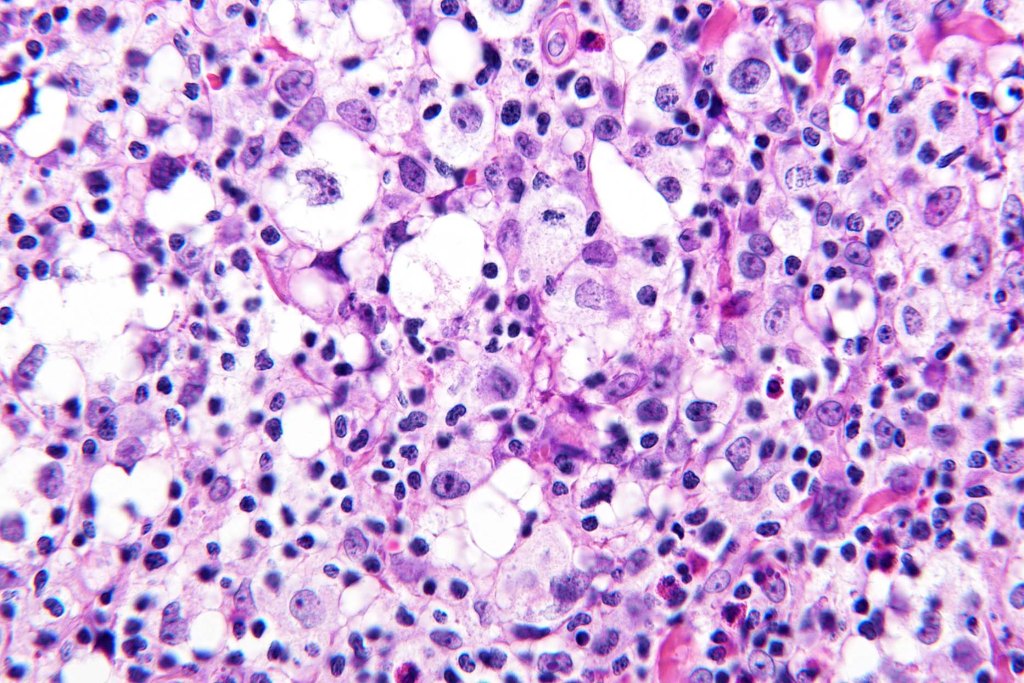
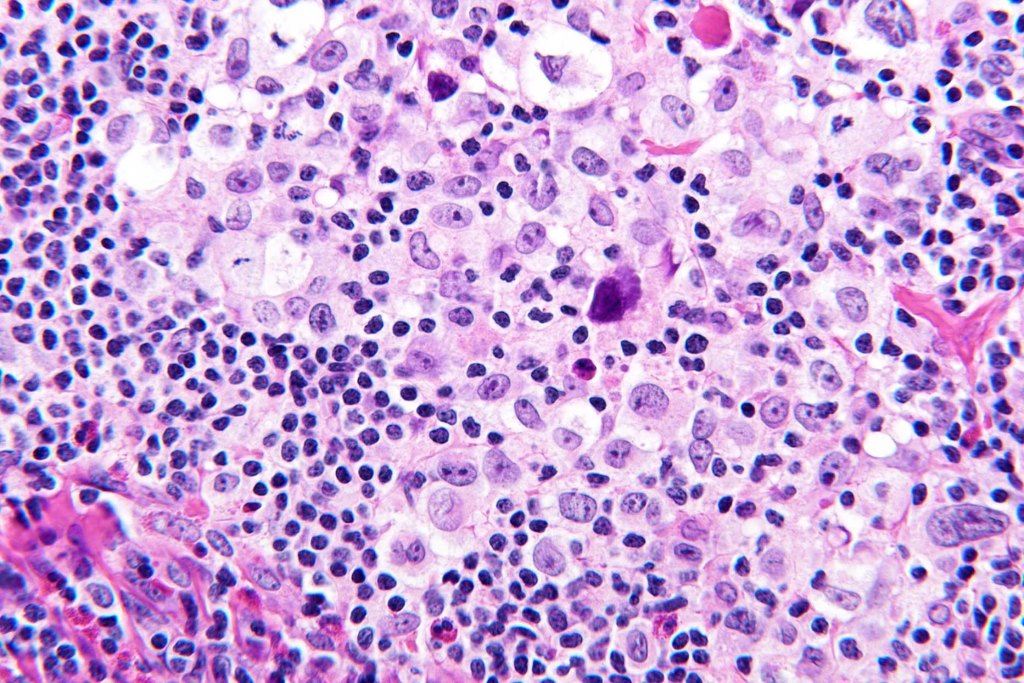
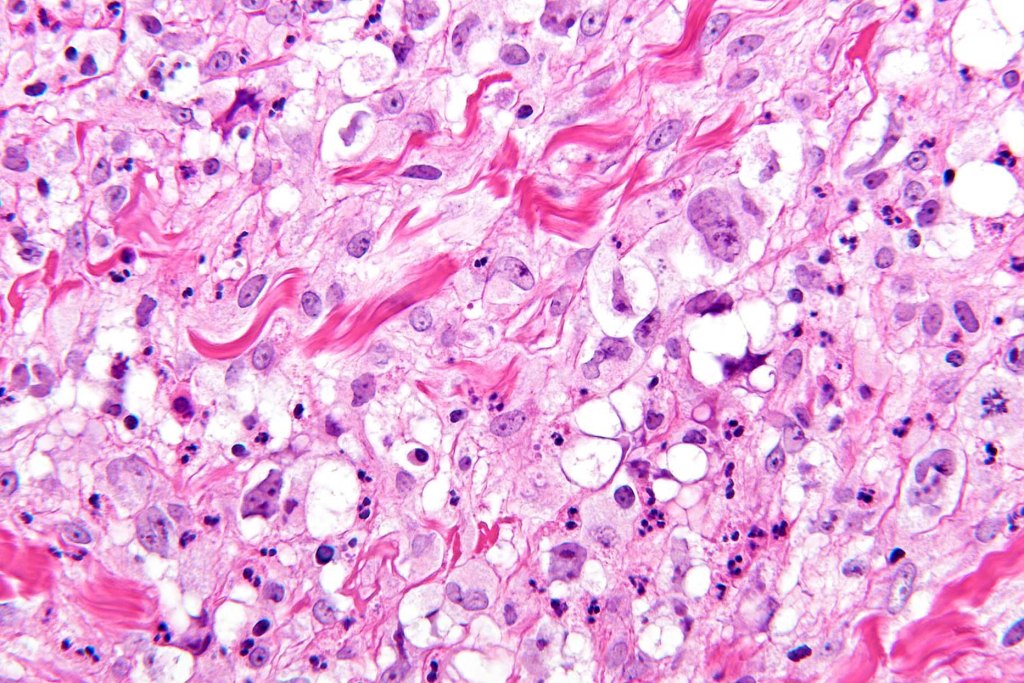
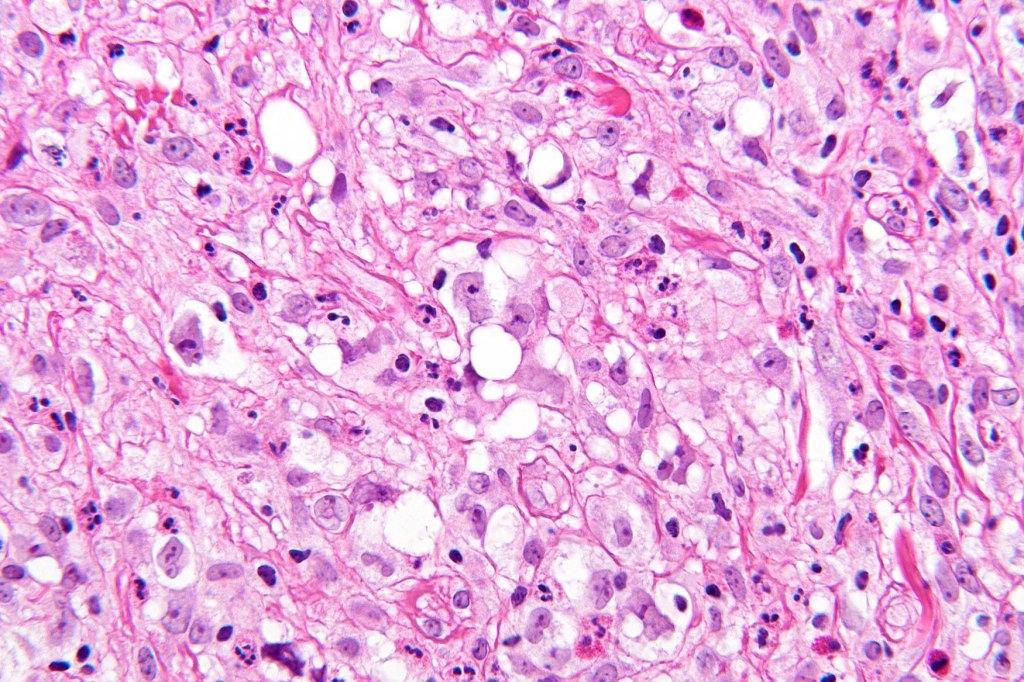
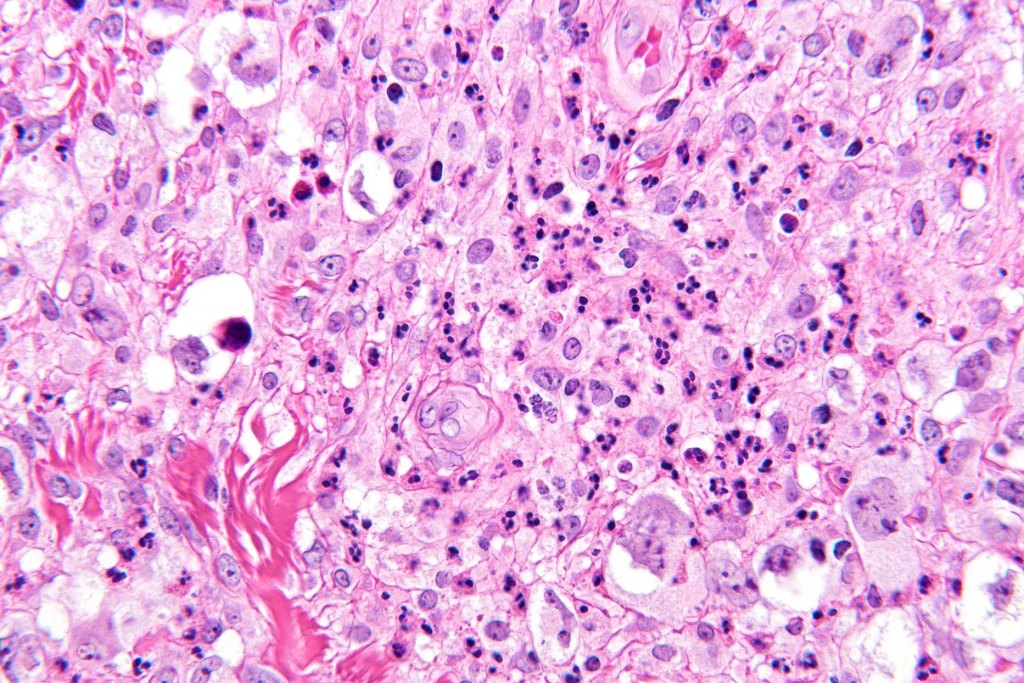
•Hodgkin & Reed-Sternberg cells- large cells with bilobed or multilobed nuclei containing a prominent nucleolus (Owl’s eye cells)
•Background population of lymphocytes, plasma cells, histiocytes, neutrophils & eosinophils
•Variable necrosis
•Variable fibrosis
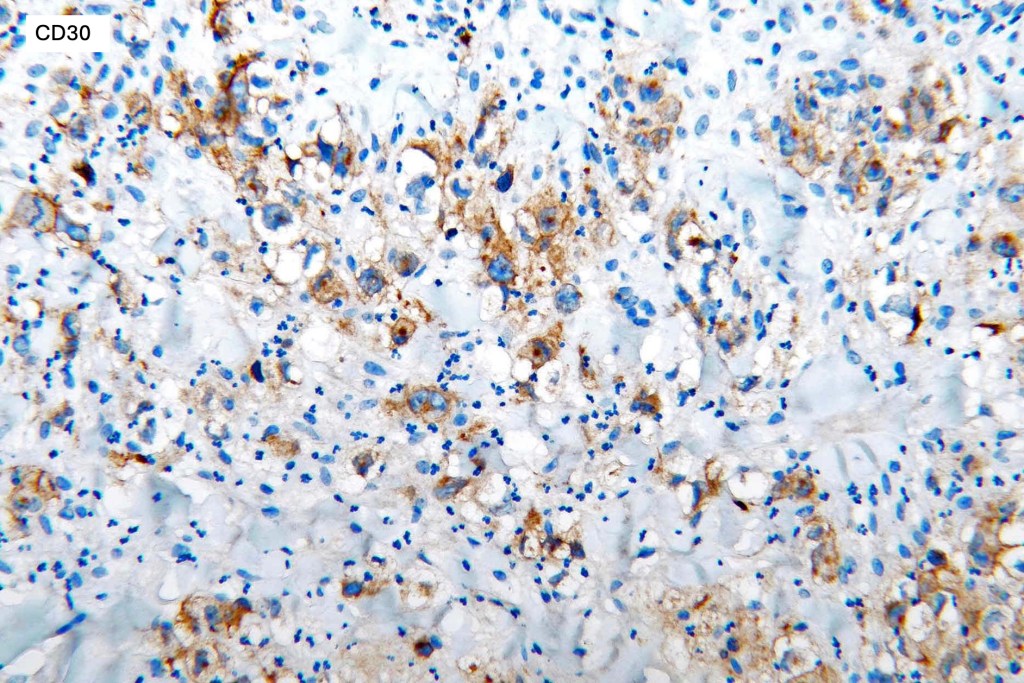
•CD30, CD15, pax 5, MUM1 +ve
•Variable weak CD20 +ve
•CD3-ve
•EMA & ALK1 –veVariable LMP1
Differential diagnosis
The main differential diagnsois with with lymphomatoid papulosis and cutaneous anaplastic large cell lymphoma. Other conditions including EBV+ mucocutaneous ulcer, diffsue large B cell lymphoma, post transplant & other immunosuppression-associated lymphoproliferative disorder. Given that secondary skin involvement only occurs in stage IV Hodgkin lymphoma, the correct diagnosis should not be in doubt.
If you liked this or the other blogs, please consider subscribing. It is free and you will receive an email everytime a new blog is posted. This is exceedingly important to me and your help would be very much appreciated. Many thanks to those who have already subscribed.

Leave a reply to Jafar taghizadeh fazli Cancel reply