This blog prepared by myself and Antonina Kalmykova is based on the review that we wrote for Pathology Outlines. I am indebted to Antonina & her technical staff for the innumerable histology cases that were scanned for me. These cases form the basis for the histology and will not be individually acknowledged unless the photogrpahs have been shared by a different friend or colleague. The clinical photographs were very kindly shared by Drs. S Vasylenko, B Lytvynenko, A Banerjee & A Kalmykova.
Clinical features
•Commonest skin cancer
•4BCC: 1 SCC
•Caucasians particularly with fair skin (types I-II Fitzpatrick phenotype)
•Predominantly a tumor of the elderly
.1.5M:1F
•Multiple tumors common
•Face, neck, trunk & proximal limbs
•Syndromic cases- xeroderma pigmentosum, albinism, Rombo, Bazex- & Gorlin syndromes
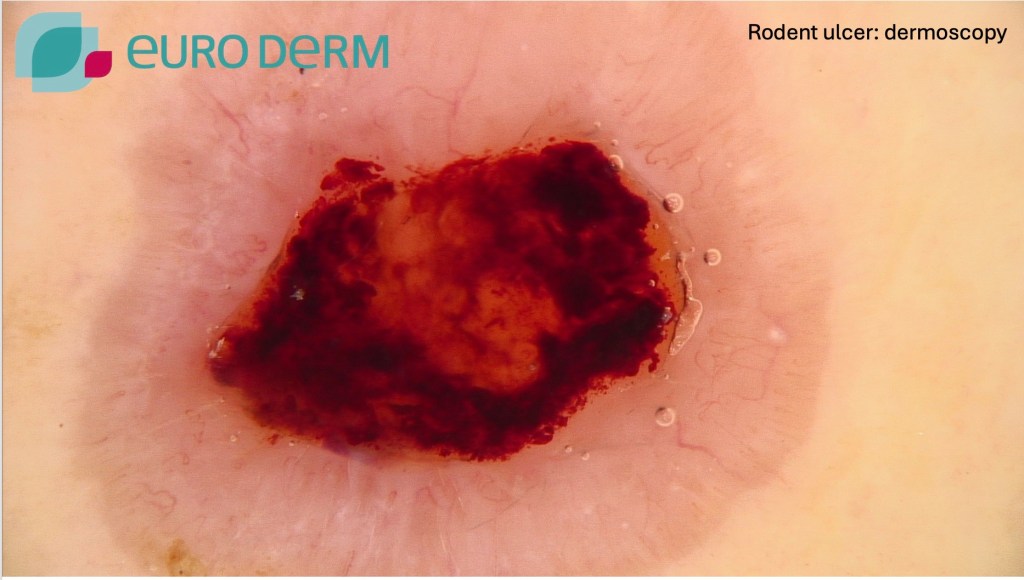
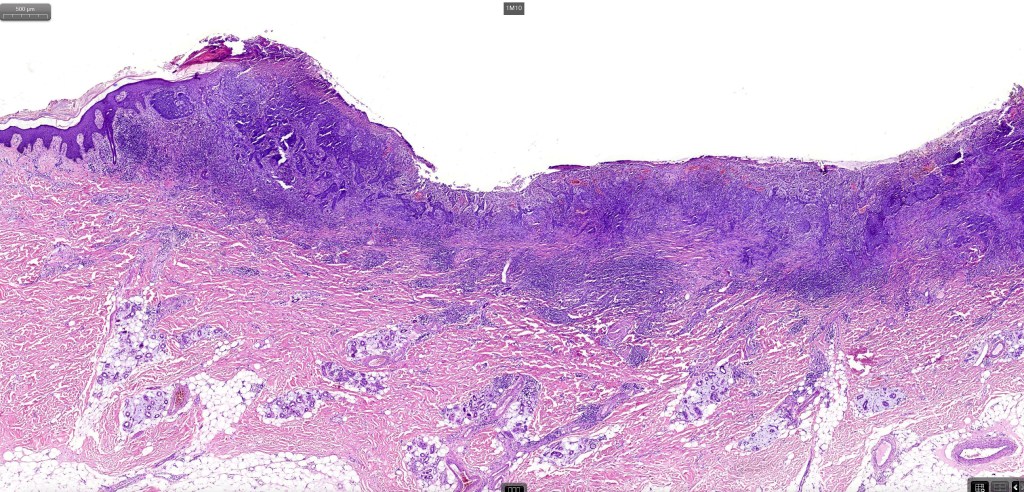
•Various clinical appearances may be encountered including ulcerative with a rolled margin (Rodent ulcer), nodular, nodulocystic, superficial, pigmented, giant, polypoid, infiltrating & morpheaform
•Fibroepithelioma is believed by some to represent a fenestrated trichoblastoma rather than a BCC
•Metastases- 0.0028-0.55% with a predilection for head & neck cases particularly with previous X-ray treatment- lymph nodes, lung, bone & skin




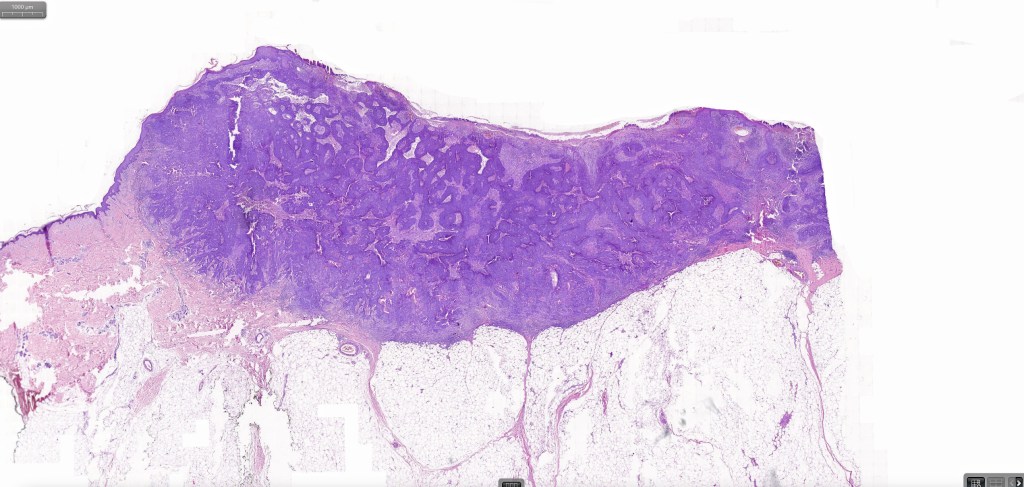
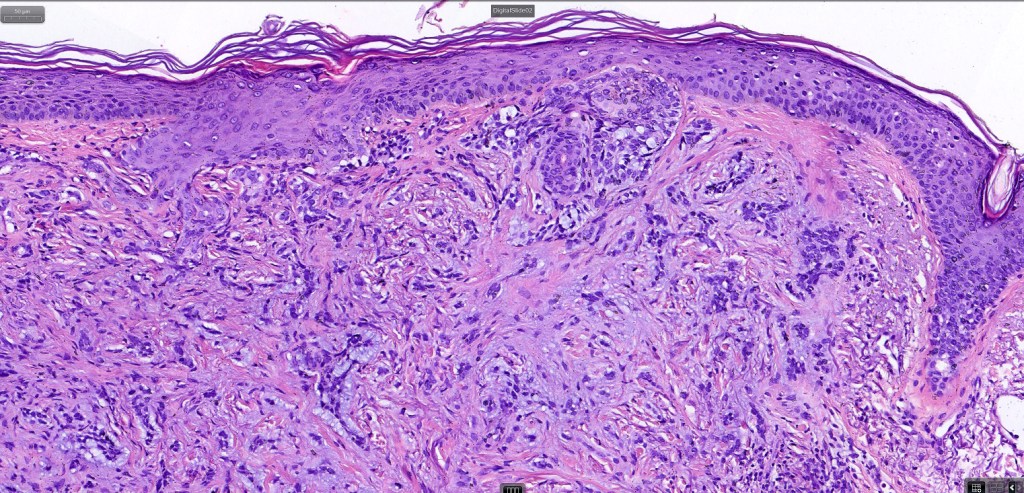
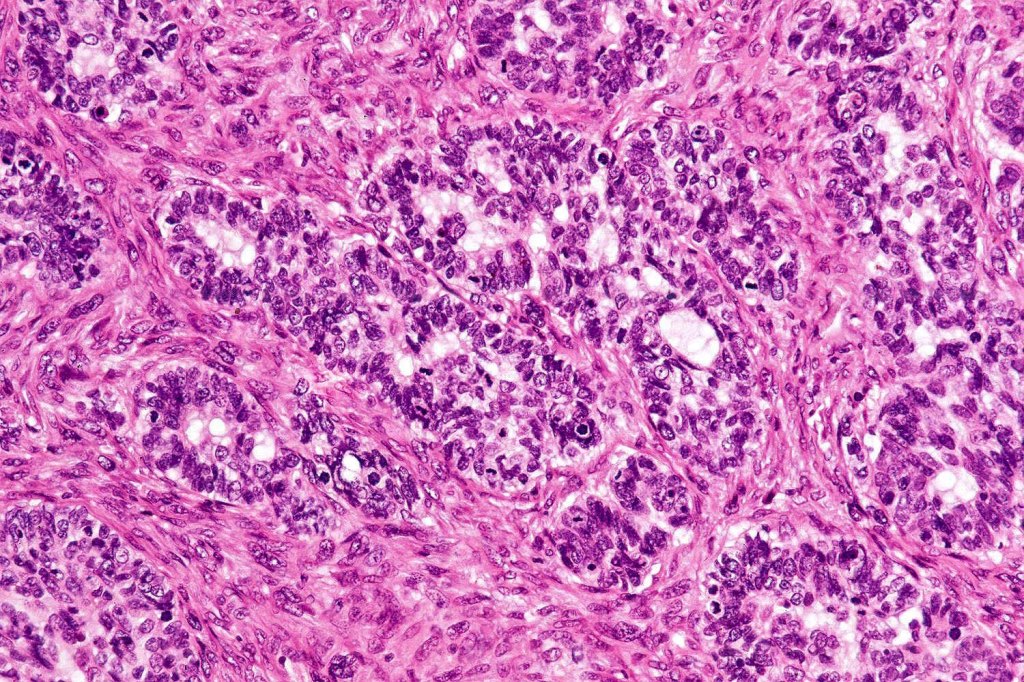
Histological features
•Mutations in the hedge-hog pathway
•Inactivating mutations involving PTCH1, PTCH2 mutations most common
•TP53, CDKN2A & RAS mutations also sometimes present
•Other important etiologies include smoking, grenz rays, ionizing radiation, coal tar, scarring dermatoses, chronic arsenic exposure & immunosuppression
•Impaired ability to repair UV-induced DNA damage
•Derives from an undifferentiated pluripotent epithelial germ cell in the follicular epithelium and interfollicular squamous epithelium
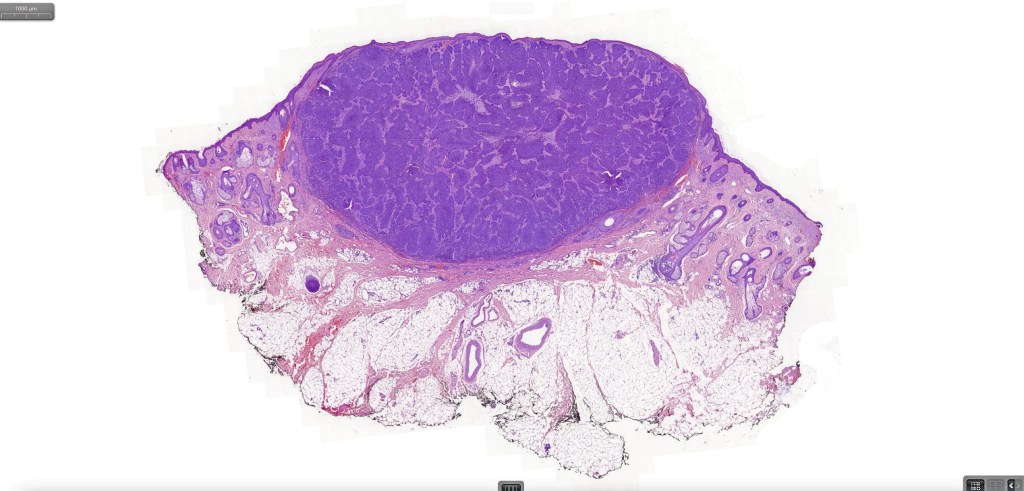
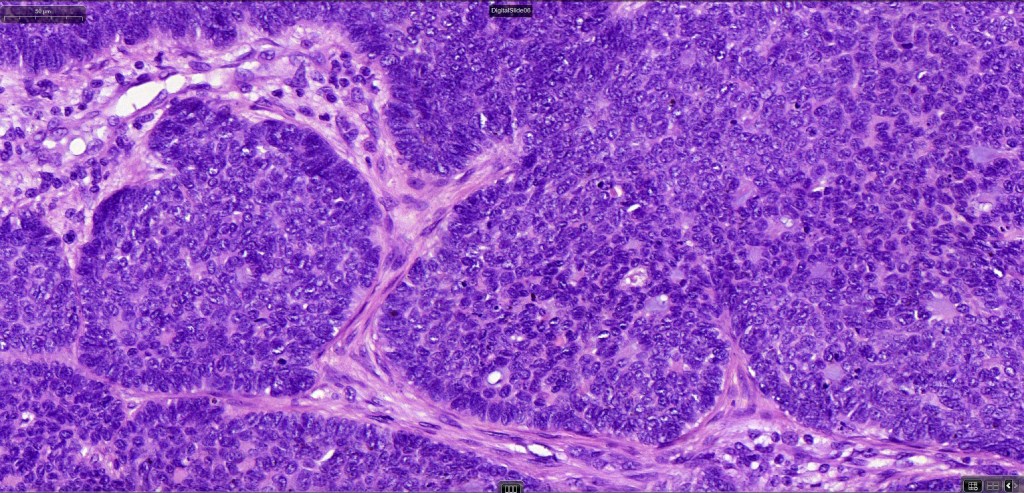
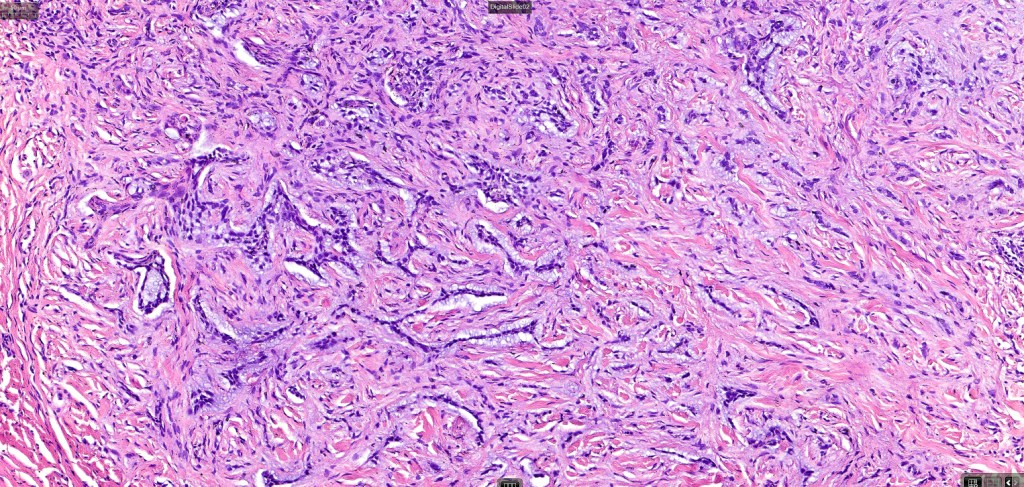
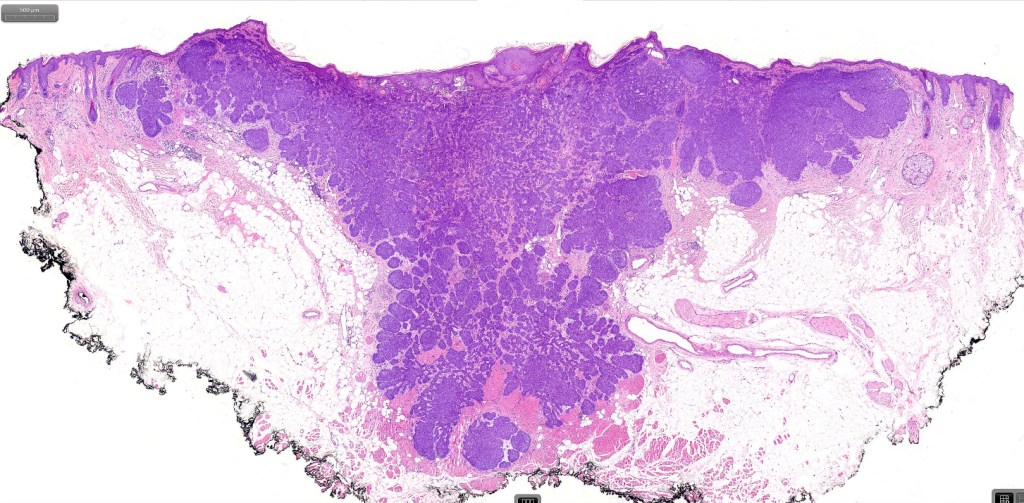
•Both epithelial & fibrous stromal components
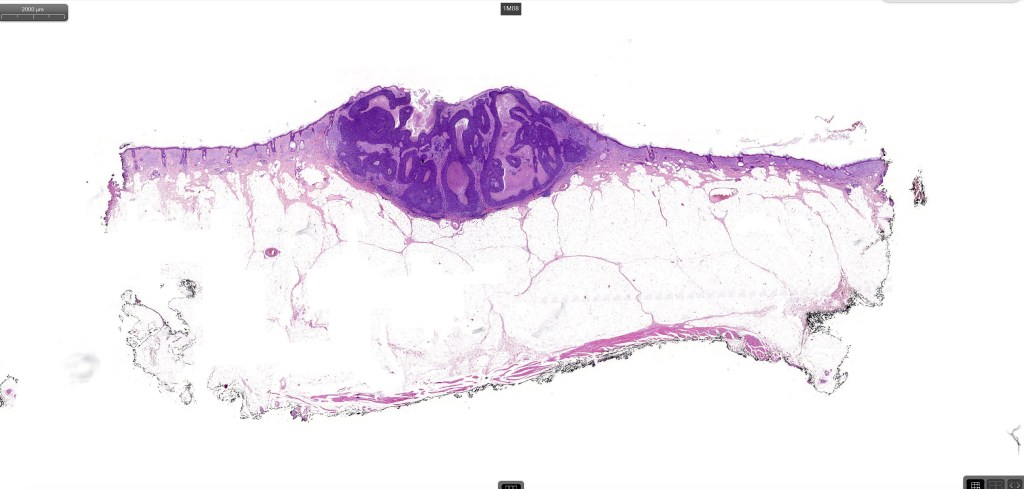
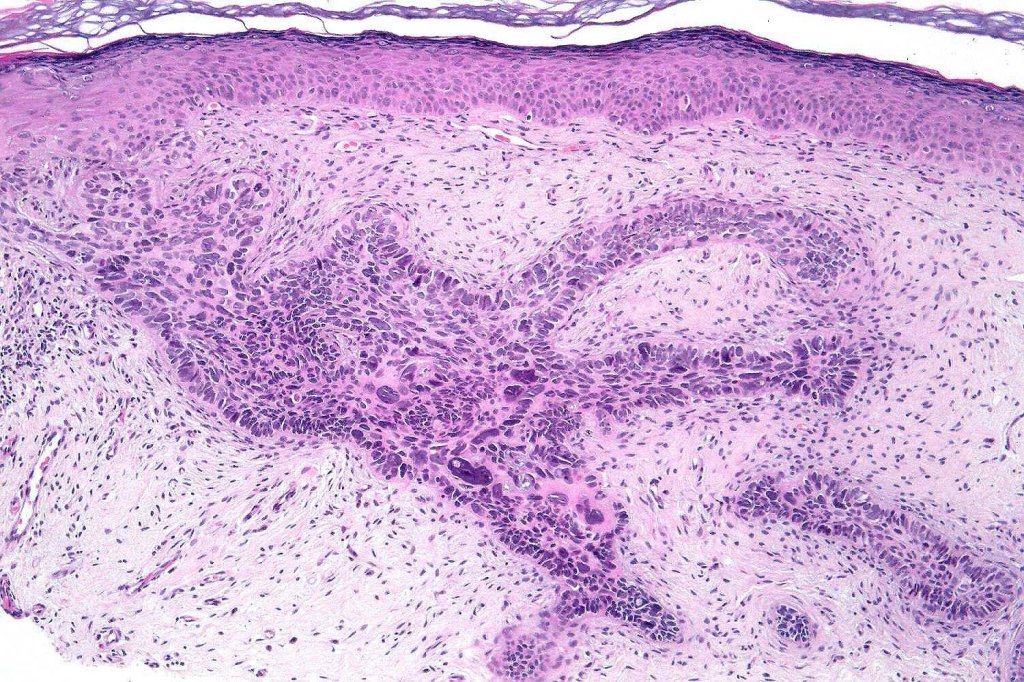
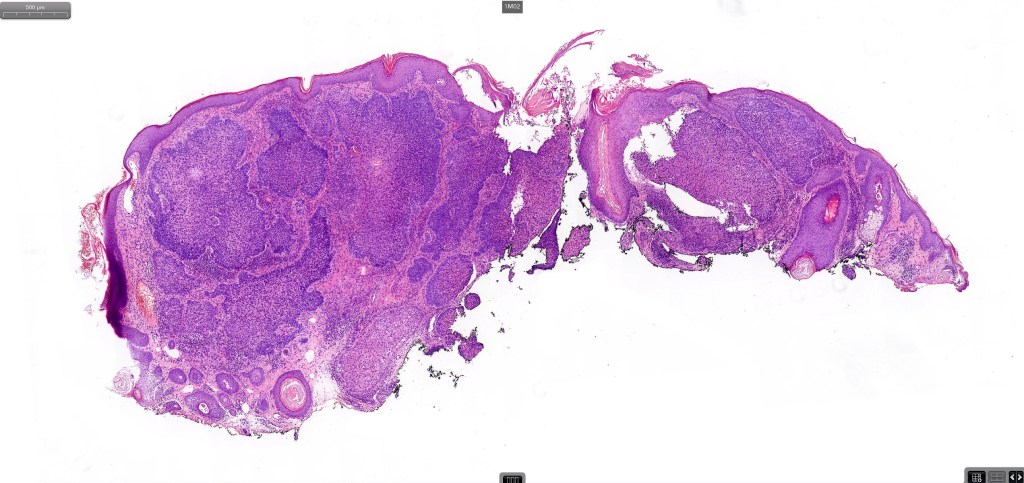
•The tumor commonly arises from the epidermis
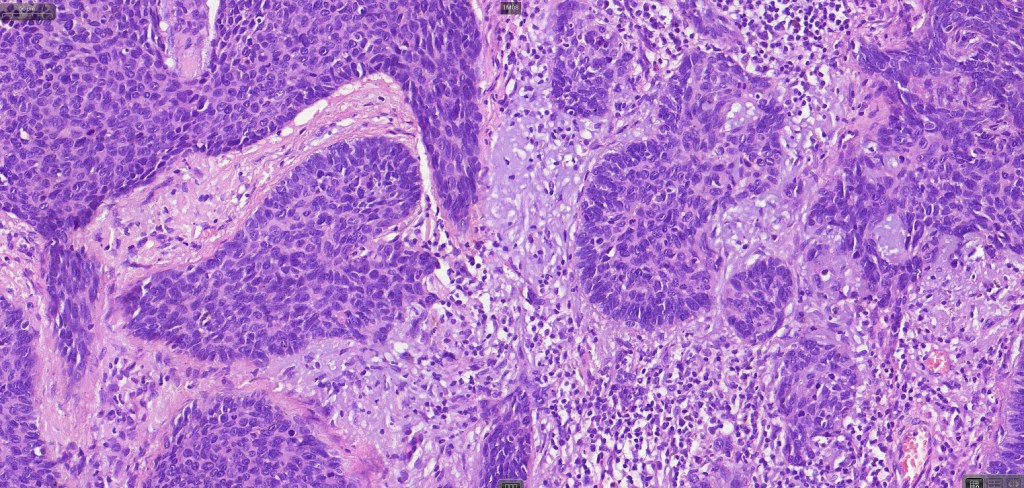
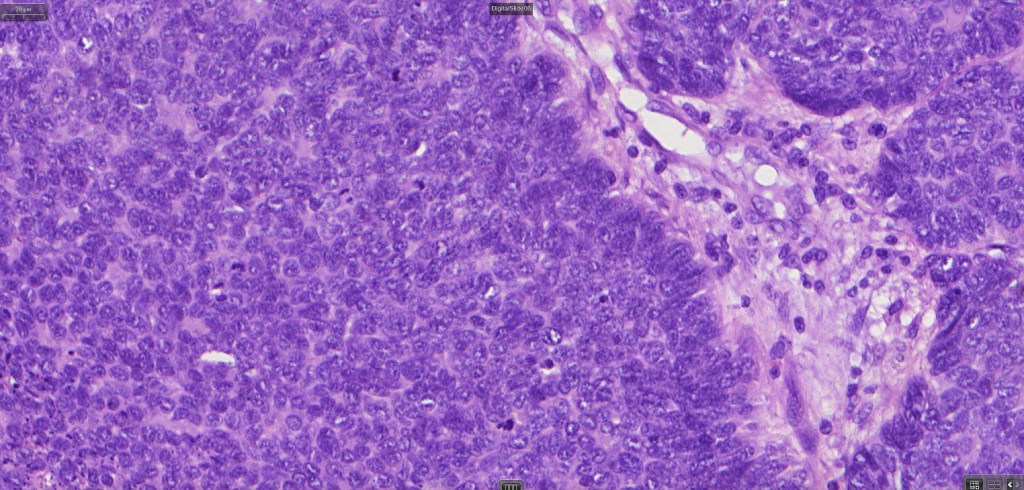
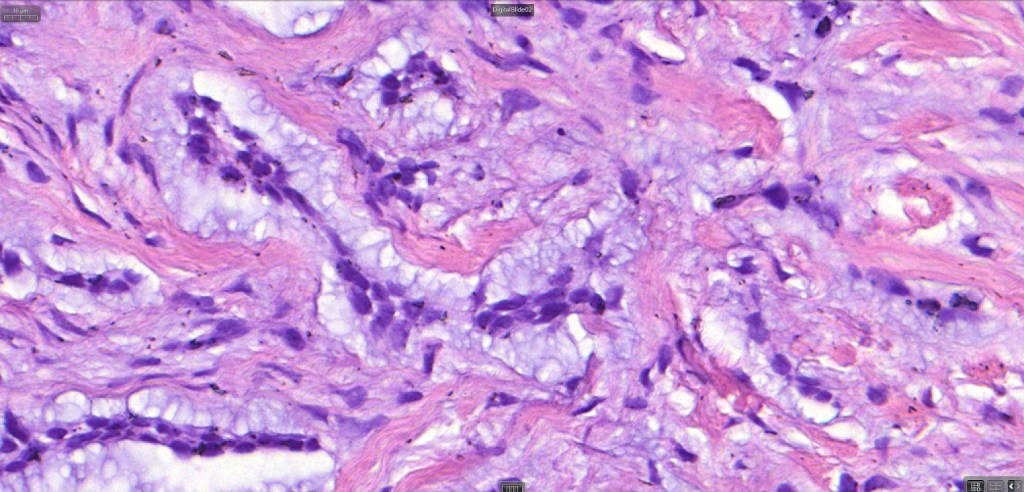
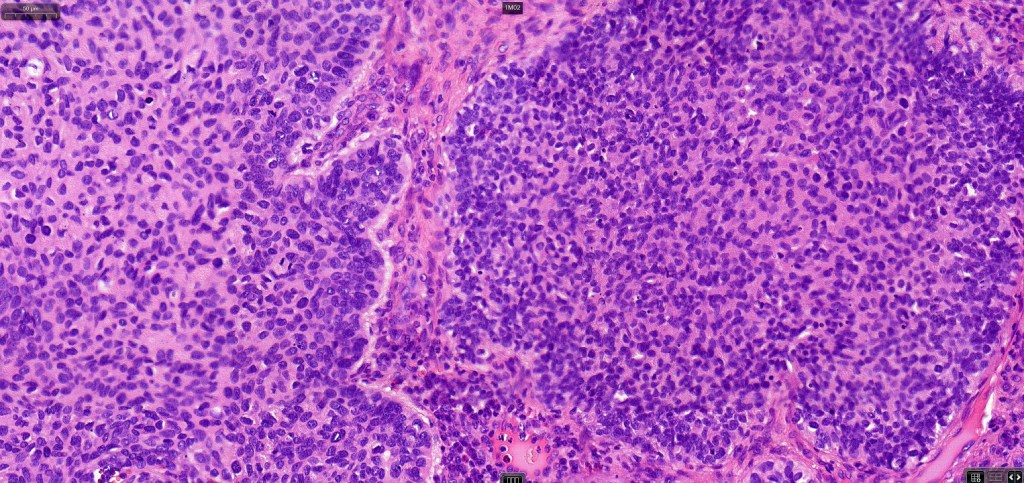
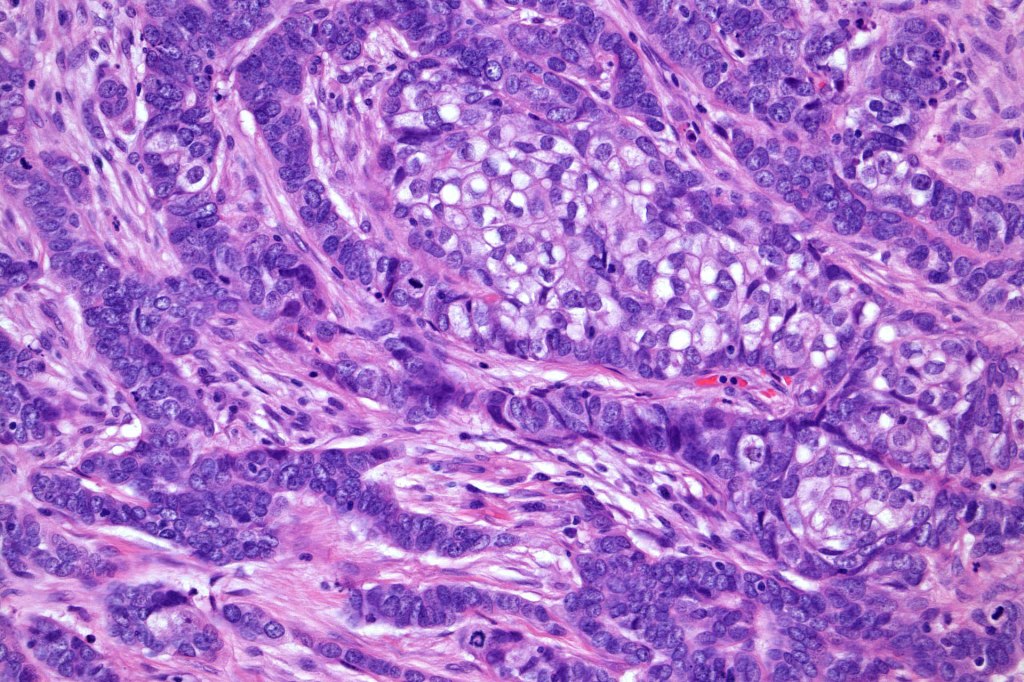
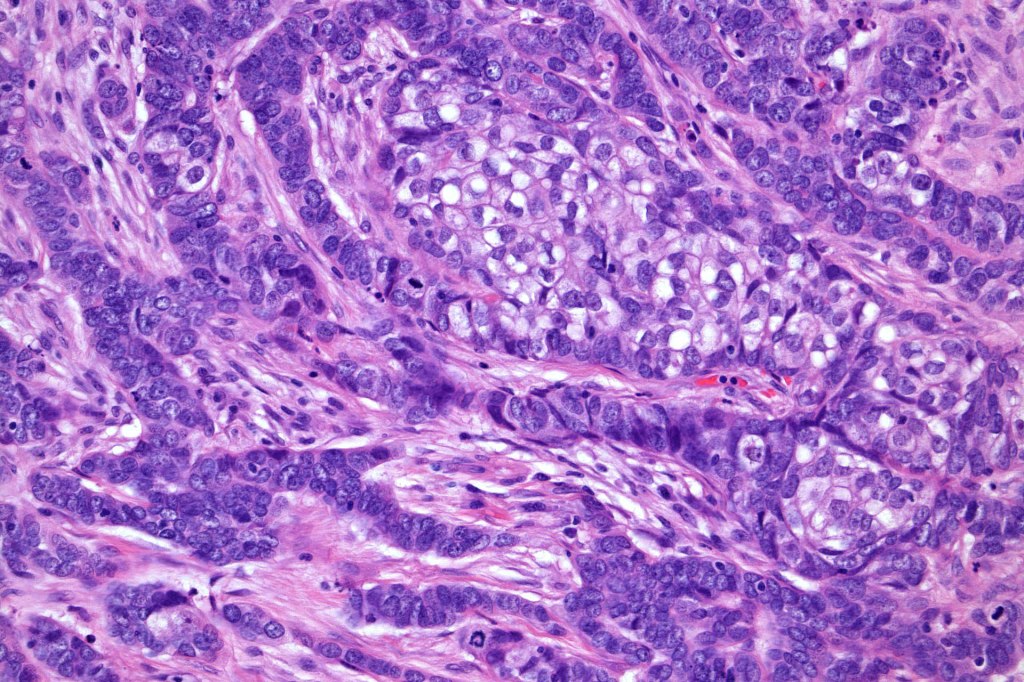
•The epithelial component is composed of uniform small, basophilic devoid of desmosomes
•Peripheral palisading
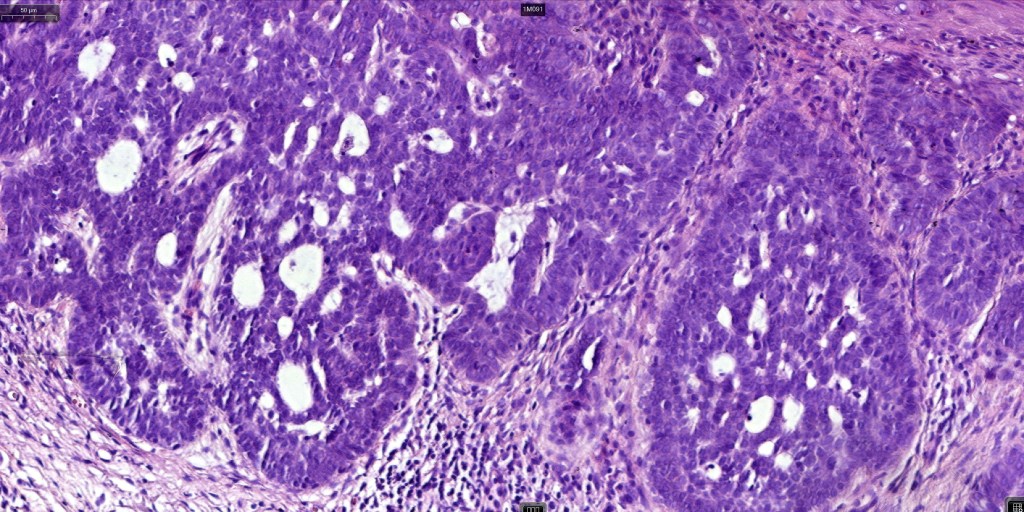
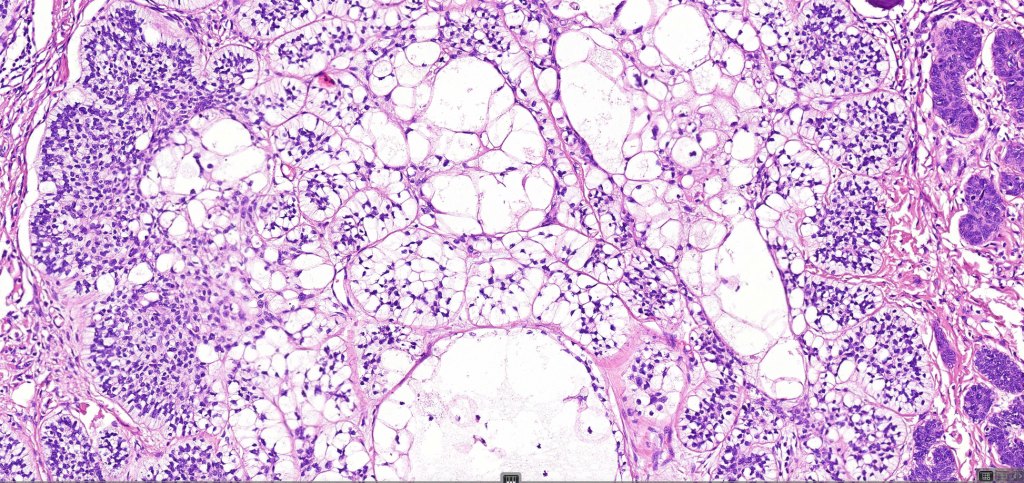
•Retraction artifact with stromal mucin
•Pseudoglandular appearance
•Mitoses often very marked
•Apoptosis
. Perineural infiltration & lymphovascular invasion sometimes present
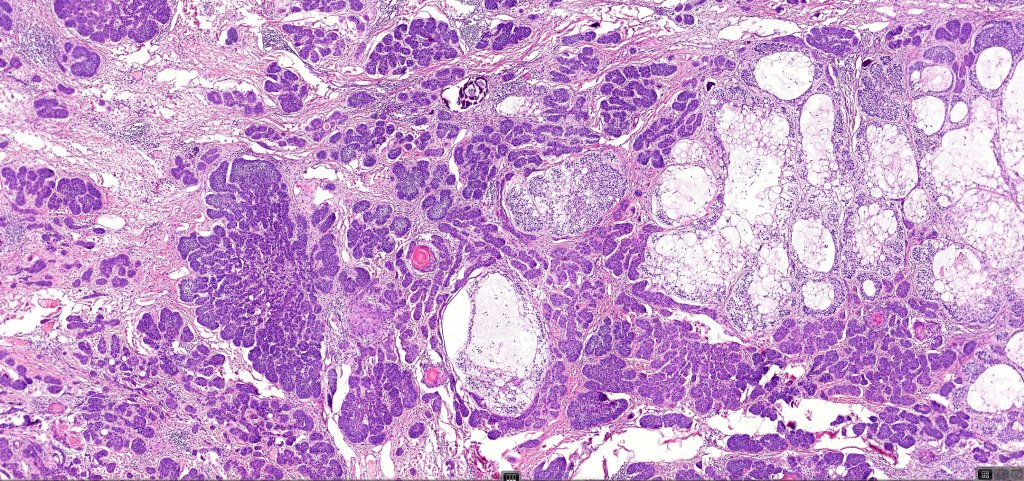
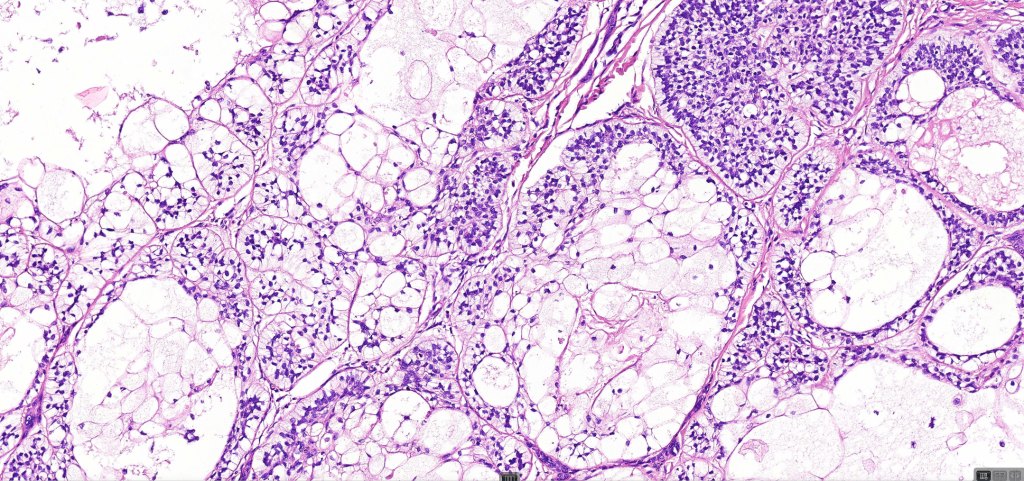
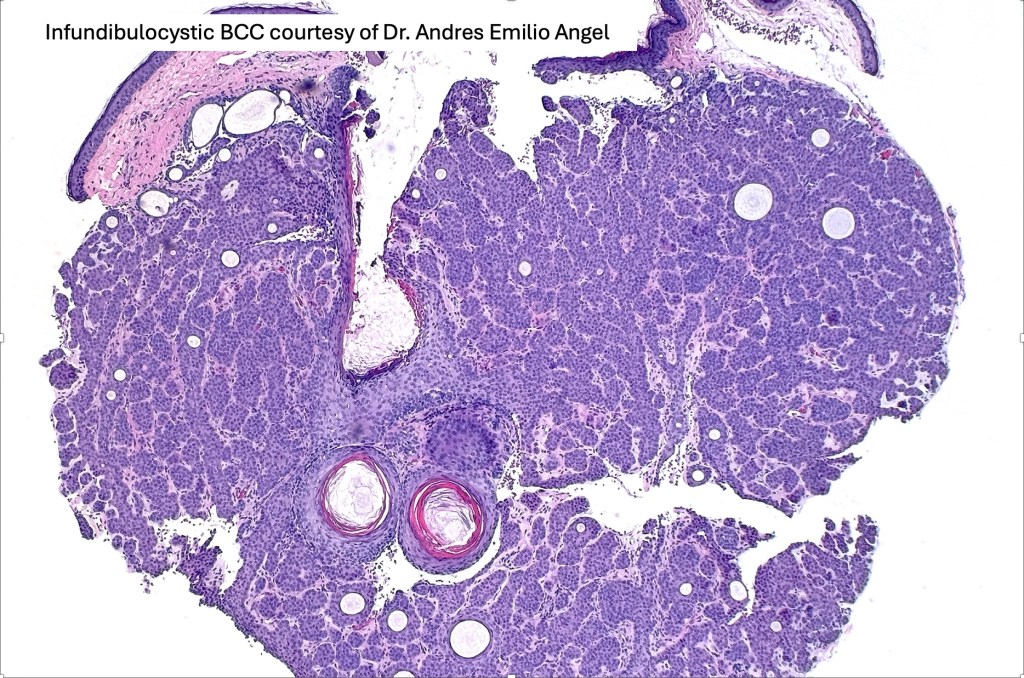
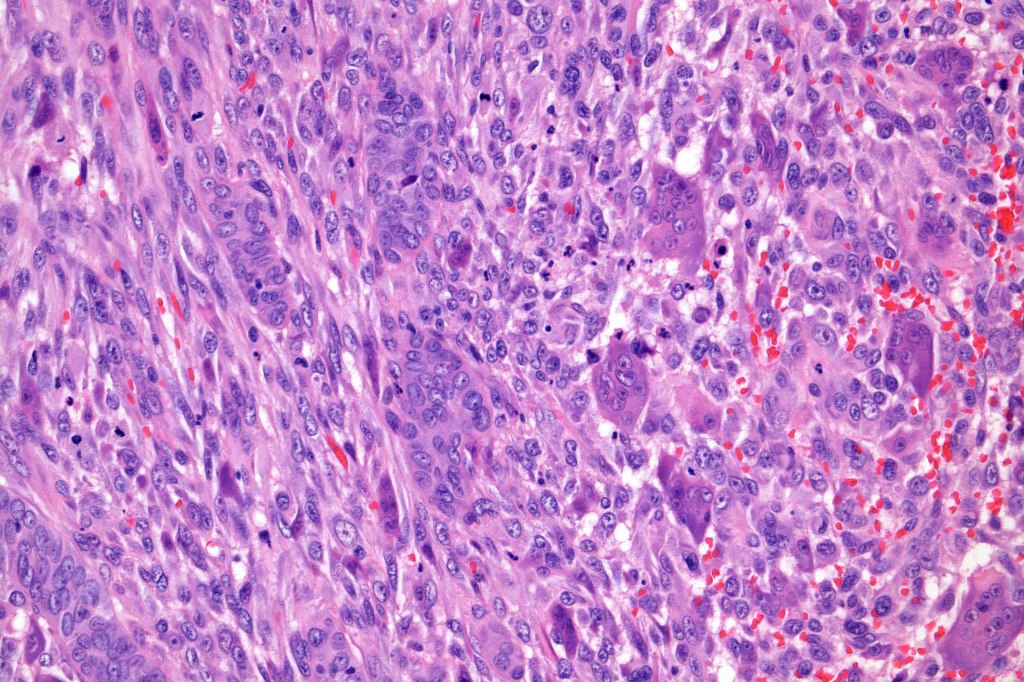
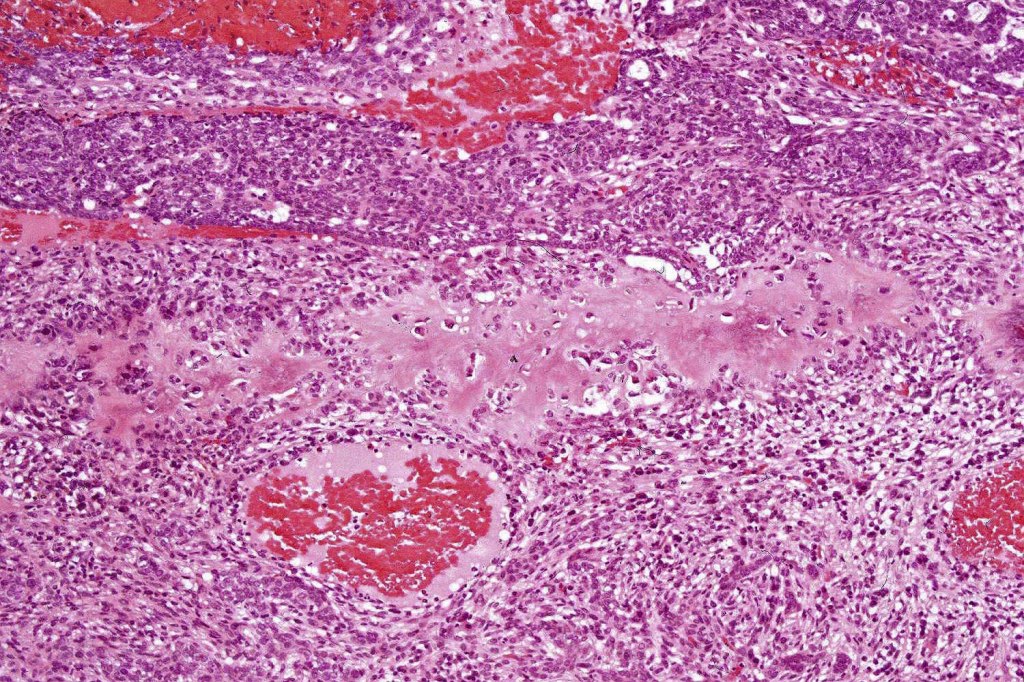
•A wide variety of histological variants are possible including nodular, nodulocystic, ulcerative, superficial, micronodular, infiltrating/infiltrative, keratotic, basosquamous, pigmented, morpheaform, keloidal, clear-cell, signet-ring cell & granular cell variants, BCC with monster cells, BCC with metaplastic features, BCC with matricial differentiation, basomelanocytic tumor (see separate blog), BCC with thickened basement membrane, BCC with carcinoid-like nuclear palisading & these are illustrated below
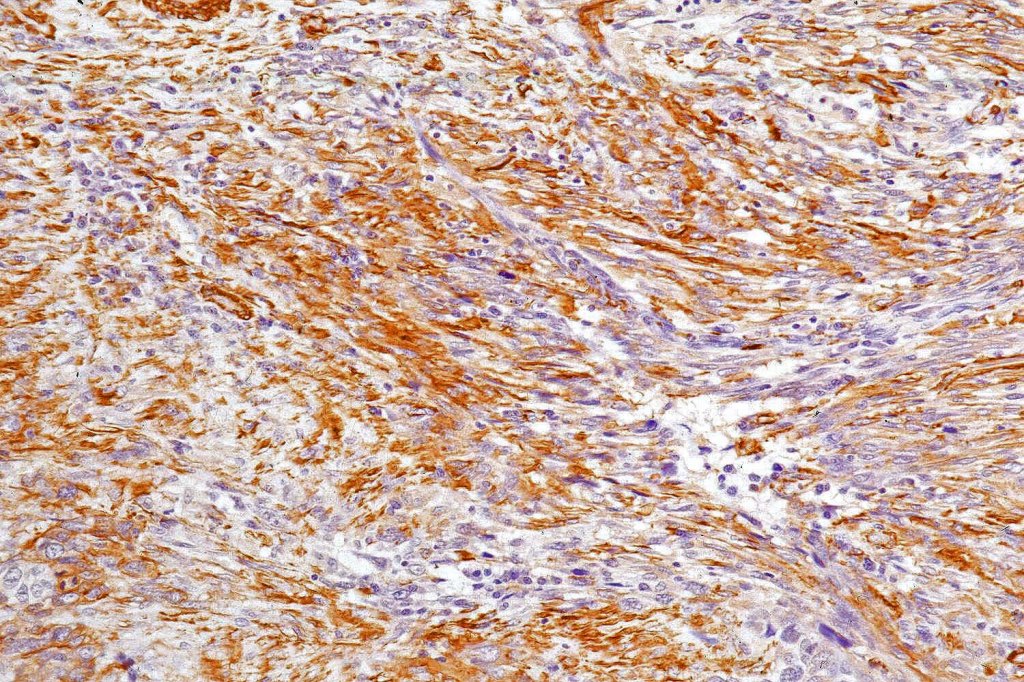
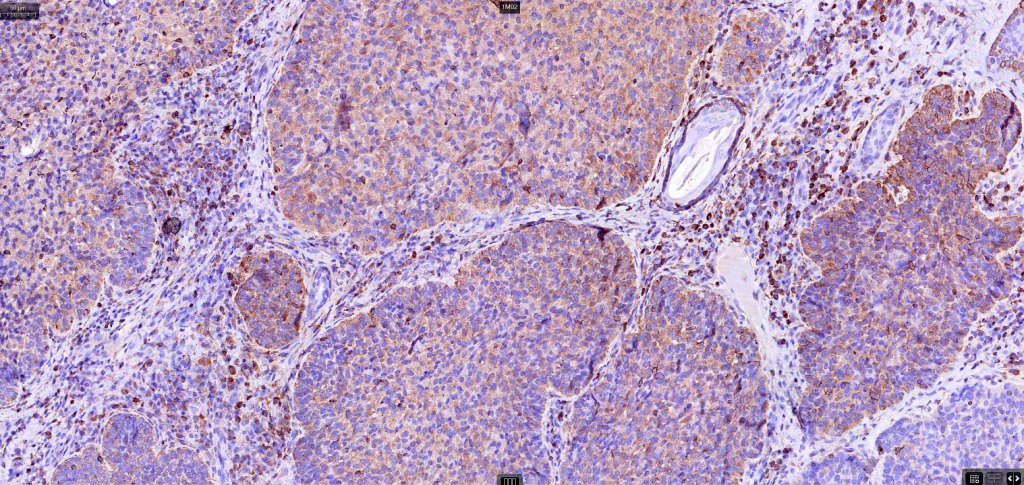
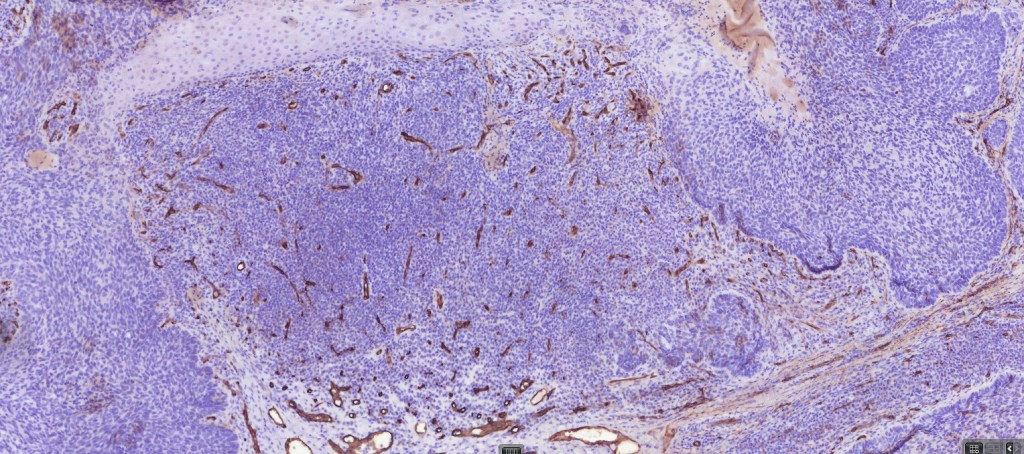
•AE1/AE3, BerEP4, p53, p63, androgen receptor, CD10 (epithelial, negative in stroma)
.EMA, CEA, CD34-ve





































Leave a comment